This is author biographical info, that can be used to tell more about you, your iterests, background and experience. You can change it on Admin > Users > Your Profile > Biographical Info page."
Cultural multiplicity is one of the major factors that contribute to breakdown of communication when carrying out health assessment. The diverse cultural factors range from religious beliefs, socioeconomic, lifestyle among others (Dains, Baumann & Scheibel, 2016). Some of the social economic explanations entail marital status and type of employment. Lifestyle issues would involve use of substance and drugs, leisure activities and in case of any taboos in their community.
When gathering information from a patient, a nurse aims at establishing a good rapport when obtaining information from the patient and giving information. Nurses and other health care providers should have certain skills and knowledge to be able to extract information from their patients (Ball et al., 2015). They should adopt a technique that wins a patient’s trust and holds him/her in high esteem. This creates a friendly environment whereby the patient is likely to give the required information adequately.
Areas that I would be sensitive when interacting with my patient would include those considered as private and sacred. Those issues would include sexual activity, pregnancy history, previous relationships and any form of abuse (Dains, Baumann & Scheibel, 2016). Failure to this would have negative impacts such as patient failing to give the required information and also the patient would have fear and be stigmatized. It would also prevent the patient from feeling discriminated.
Some of the questions that would target my patient would be as outlined below. In case of an emergency, who is the closest person who can be contacted? Are you involved in any relationship? Have you been sexually involved with a person, oral, vaginal or anal or other forms of sexual activity for the past six months? For how long have you been having the vaginal discharge and what are the characteristics? Do you have any sexual concerns you can ask? Do you feel safe with your sexuality and sexual identity? Have you ever been diagnosed with a sexual transmitted infection? Do you use alcohol or any substance when engaging in sexually activity (Sullivan, 2012)?
Dains, J. E., Baumann, L. C., & Scheibel, P. (2016). Advanced health assessment and clinical diagnosis in primary care (5th ed.). St. Louis, MO: Elsevier Mosby.
Sullivan , D. D. (2012). Guide to clinical documentation (2nd Ed.). Philadelphia, PA: F. A. Davis.
Want help to write your Essay or Assignments? Click here
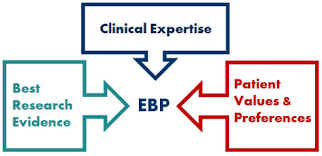
Evidence based practice is the inter-disciplinary approach that encompasses the principles of best-evidenced research, clinical expertise and client values and preferences. The evidence desired of a situation can be described as the assurity that the possibility of an event is well researched and anticipated. Evidence based practice has been popularized in the medical world for decades but was formally introduced in 1992 (Townsend, 2014).
Many students in the fields of nursing and medicine are acquired to undertake evidence-based research where they prove the existence of a phenomenon using primary data that can be considered relevant in the medical field. This implies that from time to time, research concerning issues such as medical epidemiology and the prevalence of certain conditions needs to be updated (Schneider & Whitehead, 2013).
Evidence based practice has been popularized in nursing due to the differing schools of thought on how to handle different patients. However, this particular school of thought has hardly been challenged.
Despite the importance of evidence based practice in nursing applications, there has been a challenge of determining how to implement it. Many institutions are unable to implement this program because it is quite costly and often; research on evidence based applications in medicine has not been forthcoming in new disease treatment trials. According to Melnyk & Fineout-Overholt (2011), the importance of evidence based practice in medicine stems from the fact that it has avoided professional negligence where the same has been prevalent.
In some cases, such research has completely dispelled certain notions about treatments, drug trials and even the interpretation of certain medical phenomena (Grove, Burns & Gray, 2014). Evidence based practice has led to the concept of empirically supported treatments (ESTs) that have essentially led to the standardization of efficacy treatment drugs for psychological conditions across the globe.
Impact of Evidence based practice on patient outcomes
According to Levin & Feldman (2012), evidence based practice has changed a lot of prognoses in the medical world. Patients that may not have had any hope of survival were able to get the right medication due to the fact that they were constantly offered the right medication, care and support. This was all based on recorded evidence on the success of such efforts. In particular, the insistence on evidence based practice by organizations such as the American Psychological Association, the American Occupation Therapy Association and the American Nurses Association has led to the extended medical cover of psychiatric patients.
Medical covers have over time failed to cover conditions that they felt did not have particular or specific outcomes with regard to treatment success (DiCenso, Guyatt & Ciliska, 2014). This is why it has been necessary to conduct research and prove to these care organizations that psychiatric and psychological intervention measures are indeed successful.
There have been cases where evidence based practice has led to the retraction of particular drugs from the market. For instance, the case concerning the use of Dichlorophenolindophenol (DCPIP) was researched in the United States and seen to have dire side-effects. The chemical compound was banned from being used in insecticides despite being effective and lethal (Melnyk et al, 2012).
There have been a lot of medical improvements over the past especially with regard to the standardization of medicinal tablets, the minimization of cost of healthcare as well as the universal reduction of medical challenges and issues pertaining to the proliferation of commonly practiced procedures. This has increased professionalism in the medical field to a great extend (Sandström et al, 2011). Regardless, the use of evidence based practice continues to be a skeptical issue with many doctors and nurses unable to agree on the levels of investment required.
Theoretical and clinical application of Evidence based practice
Theoretically, evidence based practice has developed into various subsets of the same school of thought. Some of these subsets include; evidence based care, evidence based treatment and evidence based learning (Godshall, 2016). With regard to evidence based care, there has been the growing concern over the need to improve nursing care in a way that can promote faster treatment and recovery of patients.
Evidence based treatment has enabled doctors to administer medication that can be supported by factual evidence concerning its side effects and prevalence for use. There has also been evidence based learning in the medical world where many students have been required to perform experimental analysis of certain phenomena in order to understand it and know how and when to apply certain medical principles (Boltz et al, 2016). This has grown the field of medicine to a great extend and indeed, it has made it possible for non-professional researchers to make medical discoveries and findings.
The clinical application of evidence based practice has majorly been in the field of clinical research. The treatment of conditions such as cancer, Alzheimer’s’ and Parkinson’s disease have required that there be new measures to prolong life and offer decent living conditions to the patients. According to Pooler (2014), there exist new discoveries in the treatment of cancer ever now and then.
This calls for universal adjustments in cancer treatments and medications. Such advancements can be very costly hence ought to be based on satiable and justifiable research. Evidence based research is thus the only confirmatory proof that the new findings do offer significant reprieve to the victims. Pearson (2014) argues that modern medicine is a lot different from traditional medicine practices where quack treatments were practiced. This is due to the propagation of evidence based research provisions.
How Registered Nurses implement Evidence Based practice
Registered nurse (RN) practice is the professional application of nursing principles and provisions. The practice is person-centred. This implies that there ought to be a personal relationship between the patient and the nurse and the nurse has to take the interests of the patient to be paramount and prioritized (Schneider & Whitehead, 2013). It is also evidence-based; implying that the practice is guided by models and theories that specify the principles of administration of care.
These models and theories can be reviewed from time to time to improve care in hospitals. The six major elements of registered nursing practice include; preventative care, curative care, formative care, supportive care, restorative care and palliative nursing care. All these elements are however based on action research principles guided by the elements of evidence based practice.
Evidence based practice has to be of a nature that can be summative in results finding as well as conclusive in the nature and type of information gathered. As a registered nurse, one is expected to perform specific duties relating to one or two of the major elements of the practice. This implies that the nurse will gain experience from a particular field as they continue to practice in it.
As a result, these nurses are expected to perform experimental treatment and diagnostic work in order to monitor certain types of diseases. For instance, in the 2014-2015 Ebola epidemics in West Africa, nurses were flown from different parts of the world to remedy the situation (Youkee et al, 2015). However, the main motivation for most of these nurses was to study the epidemiology of the Ebola virus. This led to major breakthroughs in the treatment of Ebola in subsequent years (Habich & Letizia, 2015).
Conclusion
Indeed, based on the literature surveyed, it is not possible for nurses to implement evidence based practice in the clinical setting without ample experience, training and support. This is due to the fact that evidence based practice requires one to be well versed with the provisions of proper treatment, satiable research methodologies and techniques as well as medical ethics principles that accompany such research (Mackey & Bassendowski, 2016).
It may not be prudent for an inexperienced person to undertake such research knowing that the stakes are quite high. Indeed, the cost of supporting evidence based practice is at times too much to bear and thus why institutions with medical schools are advised to have hospitals to implement this practice. All the same, it is critical to ensure that evidence based practice is applied where possible to guarantee the best results from a treatment procedure (Lipscomb, 2016).
The medical world is vast with different possibilities, treatments and medications. There is no single procedure in most applications. Old procedures are replaced with new ones and so are the tablets, injections and psychological and psychiatric therapies. The evolution of the medical world is commensurate with the evolution of human kind.
Change is the constant that keeps the universe developing towards better futures. As a result, support for research should not just be a possibility but a requirement. Evidence based practice should take precedence in all applications in the field of nursing and clinical medicine. Where this is applied, a lot of deaths will be avoided and better, cheaper and safer treatment methods will be realized.
References
Boltz, M., Capezuti, L., Fulmer, T. T., & Zwicker, D. (2016). Evidence-Based Geriatric Nursing Protocols for Best Practice, Fifth Edition. New York, NY: Springer Publishing Company.
DiCenso, A., Guyatt, G., & Ciliska, D. (2014). Evidence-based nursing: A guide to clinical practice. Elsevier Health Sciences.
Godshall, M. (2016). Fast Facts for Evidence-Based Practice in Nursing, Second Edition: Implementing EBP in a Nutshell. New York: Springer Publishing Company.
Grove, S. K., Burns, N., & Gray, J. R. (2014). Understanding nursing research: Building an evidence-based practice. Elsevier Health Sciences.
Habich, M., & Letizia, M. (2015). Pediatric Pain Assessment In the Emergency Department: A Nursing Evidence-Based Practice Protocol. Pediatric Nursing, 41(4), 198-202.
Levin, R. F., & Feldman, H. R. (2012). Teaching evidence-based practice in nursing. Springer Publishing Company.
Lipscomb, M. (2016). Exploring Evidence-based Practice : Debates and Challenges in Nursing. London: Routledge.
Mackey, A., & Bassendowski, S. (2016). Original article: The History of Evidence-Based Practice in Nursing Education and Practice.Journal Of Professional Nursing, doi:10.1016/j.profnurs.2016.05.009
Melnyk, B. M., & Fineout-Overholt, E. (Eds.). (2011). Evidence-based practice in nursing & healthcare: A guide to best practice. Lippincott Williams & Wilkins.
Melnyk, B. M., Fineout-Overholt, E., Gallagher-Ford, L., & Kaplan, L. (2012). The state of evidence-based practice in US nurses: Critical implications for nurse leaders and educators. Journal of Nursing Administration, 42(9), 410-417.
Pooler, A. (2014). An Introduction to Evidence Based Practice in Nursing & Healthcare. London: Routledge.
Sandström, B., Borglin, G., Nilsson, R., & Willman, A. (2011). Promoting the implementation of evidence‐based practice: A literature review focusing on the role of nursing leadership. Worldviews on Evidence‐Based Nursing, 8(4), 212-223.
Schneider, Z., & Whitehead, D. (2013). Nursing and midwifery research: methods and appraisal for evidence-based practice. Elsevier Australia.
Stevens, K. (2013). The impact of evidence-based practice in nursing and the next big ideas. The Online Journal of Issues in Nursing, 18(2).
Townsend, M. C. (2014). Psychiatric mental health nursing: Concepts of care in evidence-based practice. FA Davis.
Youkee, D., Brown, C. S., Lilburn, P., Shetty, N., Brooks, T., Simpson, A., & … Johnson, O. (2015). Assessment of Environmental Contamination and Environmental Decontamination Practices within an Ebola Holding Unit, Freetown, Sierra Leone. Plos ONE, 10(12), 1-10. doi:10.1371/journal.pone.0145167
Want help to write your Essay or Assignments? Click here
Decentralization is a longstanding but still developing concept that is yet to find a coherence definition and measurement model. The lack of mutual definition of decentralization and a measurement model makes it difficult to implement it and monitor the outcomes of the same in countries that have adopted it. This explores the concept of decentralization, with particular interest in Kenya which recently adopted devolution in its new Constitution of 2010.
The first part of the paper deals with the definition of decentralization. While the definition of the decentralization is still an issue, the paper defines it as the transfer of power and resources away from the central government. The concepts in this definition include ‘transfer’ and ‘decentralized system’. The second part of the paper deals with objectives.
The concepts under this subheading include; definition, measurement, and effectiveness. The third subheading is types of decentralization. This is a very important part of the paper as it distinguishes between the various designs and their effectiveness. The concepts under this subheading include; delegation, deconcentration, devolution, fiscal decentralization, political decentralization, and administrative decentralization.
The fifth subheading is on measuring decentralization. Concepts include ‘interrelated’ and ‘confirmatory factor analysis’. The paper has explored literature from various authors on the subject. The definition and types of decentralization are based on theoretical framework, while measurement is based on empirical studies.
Definition of decentralization
Whereas developing governments such as Kenya are shifting to decentralization as a way of promoting service delivery, the definition of decentralization remains an unsettled issue. In essence, there’s no mutual agreement in regards to the definition of decentralization and the manner in which decentralization should be measured. Nevertheless, most scholars refer to decentralization as the transfer of power and resources away from the central government (Schneider, 2003). A decentralized system is one in which a central authority plays a lesser role in one or all these dimensions.
Kenya is an elaborate developing country that recently adopted a devolution policy in its 2010 Constitution. The Constitution provides for fiscal, administrative and political decentralization through the creation of a new layer of county governance. The sweeping policy changes in Kenya have resulted in a new regime of governance comprising of a national government and 47 county governments (Boex & Kelly, 2011).
The 2013 elections marked the official launch of decentralization, which resulted to the election of 47 governors and county assemblies. This system of decentralization has presented both benefits and limitations in governance. The aim of decentralization in Kenya is to promote public participation in governance.
Objectives
This paper looks into decentralization with a keen eye on its definition, types and measurement models. The aim of the paper is to establish the effectiveness of decentralization in developing countries with a close interest on Kenya’s context. This paper demonstrates that decentralization is neither bad nor good when it comes to macroeconomic stability, equity, or efficiency, but rather is outcomes highly depends on institution-specific model (Litvack, Ahmad & Bird, 1998).
Types of decentralization
Care must be observed when defining decentralization since it takes different dimensions and forms. There are varied institutional restructurings encompassed in the term, decentralization, thus highlighting the possibilities of many variants operating simultaneously in a country or even a sector. When establishing different types of decentralization, it is important to distinguish among devolution, delegation and deconcentration (Litvack, Ahmad & Bird, 1998).
Devolution involves the transfer of management, financial and decision-making authority by the central government to quasi-autonomous governance units. Kenya has a devolved government, in which responsibilities for services have been transferred to county governments. County governments have power to make investment decisions and raise their own revenue.
Delegation, on the other hand, refers to a form of decentralization in which public administration functions and decision-making responsibilities are transferred from the central government to local units of government. Although these units are not entirely controlled by the central government, they have an ultimate accountability to it. In this design, the local government acts as an agent of the central government and thus aims at fulfilling the interests of its principal.
The third type of decentralization is deconcentration, which involves the transfer of certain central government responsibilities to regional units. This type does not involve the transfer of authority to local units, implying that there will be minimal limitations or benefits of decentralization to be realized.
Schneider (2003) suggests three core dimensions of decentralization: political, administrative and fiscal decentralization. These dimensions determine the degree to which intergovernmental relationships are devolved, deconcentrated or delegated (Litvack, Ahmad & Bird, 1998). Political decentralization involves the transfer of political functions of governance from the central government to regional governments.
Political decentralization theories deal with aggregation, contestation, participation, articulation, organization, and mobilization of interests. According to Fox and Aranda (1996), a decentralized political system is one in which local political issues and actors enjoy partial independence from the central authority. Administrative decentralization involves the transfer of autonomy from the central government to regional governments.
Public administration theories focusing on decentralization deal with modern bureaucracies. In the Kenyan context, the Constitution provides for devolution, which gives autonomy to the county government to exercise control and power over their territories. There are great hopes that decentralization will impact positively on service delivery, job creation and governance.
However, Kenyan citizens are not in a proper position to participate fully in governance due to difficulties encountered in accessing basic information about project implementation, expenditures, budgets, policies, and local development priorities.
Fiscal decentralization involves the transfer of fiscal impact from central government to regional authorities. Fiscal federalism theories focus on maximization of social welfare, with the ultimate goal of promoting distributive equity, allocative efficiency, and economic stability. Critics of fiscal federalism argue that fiscal decentralization focuses majorly on demand efficiency while ignoring supply efficiency (Prud’homme, 1995).
In addition, fiscal federalism assumes certain hypotheses that are not applicable in developing countries. For instance, whereas fiscal federalism assumes that taxpayers in all jurisdictions express their interests through their votes, this is not what happens in Kenya. Voters in Kenya usually cast their votes in line with their political party, tribal, or personal loyalties.
Measuring decentralization
Efforts towards measurement of decentralization are still in their formative stage (John & Chathukulam, 2003). This is because of the lack of common standards for measuring decentralization and also the little agreement concerning the very meaning of decentralization (Vengroff & Salem, 1992).
Vengroff & Salem (1992) adopted a hypothesis that decentralization leads to quality governance in developing countries. For purposes of providing an empirical ground for a comparative evaluation, the authors established a model based on the commitment, intensity and scope of decentralization in a country. In their comparative assessment, the authors found that decentralization in Tunisia resulted to good governance.
Further studies on measurement of decentralization were done in the early 21st Century by John and Chathukulam (2003) and Schneider (2003). According to Schneider (2003), the three dimensions of decentralization are closely interrelated. Nevertheless, it is not clear as to the extent to which these dimensions are interrelated. This ambiguity may cause confusion when measuring the outcomes of each dimension in a system such as Kenya where all dimensions are applied.
Schneider (2003) proposes a measurement model for decentralization. The author, however, cautions on the shortcoming of this model in regards to the likelihood of one dimension simultaneously picking up elements of the other dimensions. Confirmatory factor analysis was utilized in testing the hypothesis that all the dimensions consist of measurable indicators. Indicators for political decentralization include state and municipal elections.
Indicators for administrative decentralization include transfers and taxation as a percentage of subnational revenues and grants. Indicators for fiscal decentralization include county revenues and expenditures as percentage of national revenues and expenditures respectively.
Conclusion
Effective decentralization can be achieved if there are sufficient resources and powers from the central government, and measures are implemented to enhance accountability of bureaucrats to elected representatives and accountability of representatives to the citizenry (Manor, 1995).
Accordingly, a properly balanced decentralized system can produce such benefits as reduced absenteeism by local government officials, reduced corruption, enhanced two-way information flow between the government and the public, increased public participation in governance, and greater responsiveness (Speer, 2012). On the other hand, decentralization has such limitations as the inability to promote poverty alleviation.
References
Boex, J., & Kelly, R. (2011). Fiscal Decentralization in Kenya: A Small Step or Giant Leap?.
John, M. S., & Chathukulam, J. (2003). Measuring decentralisation: the case of Kerala (India). Public Administration and Development, 23(4), 347-360.
Fox, J. A., & Aranda, J. (1996). Decentralization and rural development in Mexico: community participation in Oaxaca’s Municipal Funds Program. Center for Global, International and Regional Studies.
Litvack, J. I., Ahmad, J., & Bird, R. M. (1998). Rethinking decentralization in developing countries. World Bank Publications.
Manor, J. (1995). Democratic decentralization in Africa and Asia. IDS bulletin, 26(2), 81-88.
Prud’Homme, R. (1995). The dangers of decentralization. The world bank research observer, 10(2), 201-220.
Schneider, A. (2003). Decentralization: conceptualization and measurement. Studies in Comparative International Development, 38(3), 32-56.
Vengroff, R., & Salem, H. B. (1992). Assessing the impact of decentralization on governance: a comparative methodological approach and application to Tunisia. Public administration and development, 12(5), 473-492.
Want help to write your Essay or Assignments? Click here
In recent times, scientific underpinnings to practice have become a major issue of concern where those performing roles in the nursing field are required to self-assess themselves for preparedness. Doctor of Nursing Degree was conceived with the objective of accelerating the translation of evidence and research into practices and also improvement of practices into expertise levels (Wysocki et al, 2015). It is essential to have a self-assessment as a DNP nurse so as to reflect on the experiences.
The reflection would entail the linkage of previous learning and the current experiences. The purpose of reflection is to gauge the extent of preparedness to advance in the nursing practice through exhibiting some advanced level skills and personal development. Through reflection, evaluation and synthesizing of information regarding the nursing practice contributes to one’s growth and development while also controlling an individual’s learning.
AACN approved the DNP for the advanced practice nurses who would be required to have sophisticated skills that would be implemented and used in the performance of their roles (Wysocki et al, 2015). The curricular competencies and essential elements in the DNP program are clearly outlined in the AACN. It is necessary to carry out a personal reflection to assess the compliance to these essentials and possession of competencies crucial for nursing practices.
Scientific underpinnings to practice are one of the essentials provided by the AACN which requires DNP graduates to have a reflection to evaluate the outcome competencies after completing the degree program (Wysocki et al, 2015). One of the competencies I would reflect on as per the scientific underpinnings to practice is the development of the care delivery approaches crucial during the performance of roles.
Assessment and reflection while considering the essentials for competencies in safety and quality patient care are another factor I would address where accountability is ensured (Kesten, 2015). The final competency is the ability to evaluate and develop effective strategies during management of the ethical dilemmas. The reflection would address these essentials of the scientific underpinnings to practice which informs the extent of preparedness.
To meet the pertinent DNP competencies, I would be required to possess some abilities, knowledge and vital skills essential for nursing practices. The DNP has been helpful in the integration of attitudes, informatics skills, and knowledge which culturally support evidence-based and culturally sensitive practices at high levels in the nursing field e.g. the leadership level (Kesten, 2015). My self-assessment after completion of the course, reflects on the competencies of the DNP as outlined by the AACN.
The learning outcomes and competencies outlined would form the basis of the self-evaluation. My increased sensitivity to different populations and diverse organizational cultures and improvement in communication skills are some of the skills identified after self-assessment which meet the pertinent competencies of the DNP (Hallas et al, 2012). These skills are essential learning outcomes for an accountable DNP graduate.
The self-assessment also helped me evaluate my enhanced skills in leadership and also handling complex clinical issues that are increasing over time. The enhanced knowledge to improve patient outcomes and nursing practice was also acquired. Through the self-assessment, I was able to evaluate the vital knowledge acquired after the DNP program. I was prepared to influence and design the best healthcare policy options with the focus on various factors such as quality, accessibility, and cost (Hallas et al, 2012).
Other factors focused on are safety, equity, efficacy and proper regulations. The acquisition of this knowledge and competencies is pertinent for a DNP graduate. After completion of the learning course in DNP, more insight on how to integrate theory and practices with the aim of ensuring quality care to all was gained. The self-assessment was important for me as it helped me evaluate my abilities in analyzing practice data and effective evaluation of outcomes in the nursing field.
The integrative abilities in implementing the nursing interventions based on science are pertinent to the DNP competencies which are an indicator of the benefits of learning the course (Hallas et al, 2012). The massive benefits in the form of skills, knowledge, and abilities gained after learning the course as identified through the self-assessment are pertinent to the DNP competencies (Terhaar et al, 2016).
The orientation program for new students is essential in impacting success positively. Having gone through the orientation program as a new student, I would gain more insight and a lot of information essential in enhancing my success at Chamberlain (Price et al, 2015). The orientation is important for me as I can acquire fundamental information needed to connect with people that would influence my success in Chamberlain.
Through the orientations, insight and a better understanding of skills and belief essential for progressing well thus influencing success while in Chamberlain is efficiently gained. Crucial information on the survival tactics and handling complex issues enhance personal growth and academic success (Price et al, 2015).
In a nutshell, it is important for everyone who undergoes the DNP degree program to ensure the best skills, abilities and knowledge is acquired after completion of the course. Such efforts would ensure the competencies gained impact the nursing practice positively.
The pertinent DNP competencies are essential due to the impacts it has brought to the nursing field by enhancing the development of both effective strategies during management of the ethical dilemmas and care delivery approaches crucial during the performance of roles (Price et al, 2015). The adoption and integration of these competencies into practice would revolutionize the nursing field for the better.
References
Hallas, D., Biesecker, B., Brennan, M., Newland, J. A., & Haber, J. (2012). Evaluation of the clinical hour requirement and attainment of core clinical competencies by nurse practitioner students. Journal Of The American Academy Of Nurse Practitioners, 24(9), 544-553. doi:10.1111/j.1745-7599.2012.00730.x
Kesten, K. S. (2015). Assessment of APRN Student Competency Using Simulation: A Pilot Study. Nursing Education Perspectives, 36(5), 332-334. doi:10.5480/15-1649
Price, D. M., Buch, C. L., & Hagerty, B. M. (2015). Measuring Confidence in Nursing Graduates Within the Framework of the AACN Essentials. Nursing Education Perspectives, 36(2), 116-117. doi:10.5480/13-1162.1
Terhaar, M. F., Taylor, L. A., & Sylvia, M. L. (2016). The Doctor of Nursing Practice: From Start-Up to Impact. Nursing Education Perspectives, 37(1), 3-9. doi:10.5480/14-1519
Wysocki, Kenneth, Patricia C. Underwood, and Susan Kelly-Weeder. 2015. “An essential piece of nursing’s future: The continued development of the nurse practitioner as expert clinician and scientist.” Journal of the American Association of Nurse Practitioners, April. 178-180. Academic Search Premier, EBSCOhost (accessed September 2, 2016).
Want help to write your Essay or Assignments? Click here
In recent times, adoption of continuous quality improvement has become essential especially in issues concerning health promotion. In this case, health organization has taken the initiative to adopt the system which helps in refinement and regular reflection to enhance better outcomes and processes to enhance quality healthcare services (Davis et al, 2014).
There are substantial benefits of integrating continuous quality-improvements and its operations in healthcare. Continuous quality improvements are important as it ensures improved communication with external and internal resources in an organization such as the community and funders. Implementation of continuous quality improvements enhances proactive processes that solve and recognizes major problems thus ensuring the care systems are predictable and reliable in nature (Davis et al, 2014).
Such measures would ensure errors are addressed, and quality is fully observed. Continuous quality-improvements are also vital as its implementation leads to more efficient clinical and managerial processes.
Continuous quality-improvements also ensures reduced costs especially those associated with poor outcomes, process failures, and errors. Through continuous quality improvements, there is the higher satisfaction of patients and others receiving healthcare services since customer satisfaction is one of its primary components (Davis et al, 2014). Other than the public health area, the continuous quality improvements are adopted and used in the social services sector. In such scenarios, firms use the tool to ensure positive outcomes are received in the business environment.
An example is when it is implemented so as to ensure continuous access to sources of funds and improving services for customers. The continuous quality-improvements are also implemented in the information technology field mostly during planning and management of information systems thus ensuring valuable information is acquired to inform the right strategies for development (Davis et al, 2014).
Reference
Davis, M. V., Mahanna, E., Joly, B., Zelek, M., Riley, W., Verma, P., & Solomon Fisher, J. (2014). Creating Quality Improvement Culture in Public Health Agencies. American Journal Of Public Health, 104(1), e98-e104. doi:10.2105/AJPH.2013.301413
Want help to write your Essay or Assignments? Click here
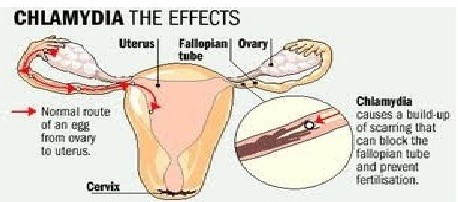
According to the Centers for Disease Control and Prevention (CDC, 2016), chlamydia is one of the common sexually transmitted infections (STIs). It is caused by Chlamydia trachomatis bacterium that damages women reproductive system. While the signs are mild, severe complications can lead to irreversible issues such as infertility. In addition, e Chlamydia may cause discharge from the male sexual organs.
Chlamydia effects
Figure 1: Chlamydia Effects
Risk factors
Some of the factors that increases the risks of contracting chlamydia are; people below 24 years; engaging in unprotected sex; various sexual partners; and previous history of STIs.
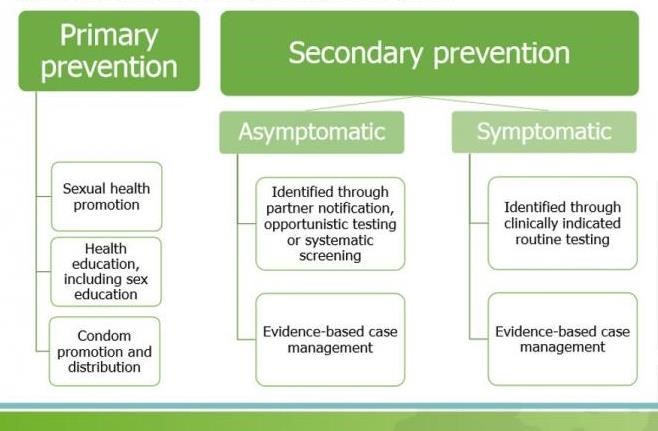
Prevention
The effective approach of preventing transmission is abstaining from sexual behaviour or being involved in a monogamous relationship with uninfected partner. Male condoms if used correctly and consistently can significantly minimize the risks of transmitting chlamydia (CDC, 2016). Moreover, it is recommended for all active sexually female below 24 years to undertake annual screening for chlamydia. Older female with risk factors for this disease are required to undergo annual screening.
Pregnant women must also undergo screening. Screening is considered the best prevention approach since a number of reproductive complications associated with chlamydia are common among women and its symptomatic. Additionally, genital signs such as discharge, a rash, sores or burning sensation during urination is an indication to seek medical advice.
In the event that an individual has been treated for this disease or other types of STIs, he or she must notify their sex partner to be treated by a health care specialist. This is important, particularly, when it comes to minimizing the risk severe complications while reducing the chances of being re-infected. Such a person and his or her sexual partner must abstain from sex till they finish treatment.
chlamydia prevention
Figure 2: Chlamydia Prevention
Prevention
The surest way to prevent chlamydia infection is to abstain from sexual activities. Short of that, you can:
Use condoms. Use a male latex condom or a female polyurethane condom during each sexual contact. Condoms used properly during every sexual encounter reduce but don’t eliminate the risk of infection.
Limit your number of sex partners. Having multiple sex partners puts you at a high risk of contracting chlamydia and other sexually transmitted infections.
Get regular screenings. If you’re sexually active, particularly if you have multiple partners, talk with your doctor about how often you should be screened for chlamydia and other sexually transmitted infections.
Avoid douching. Douching decreases the number of good bacteria in the vagina, which can increase the risk of infection.
Two-thirds of new chlamydial infections occur among youth aged 15-24 years.3It is estimated that 1 in 20 sexually active young women aged 14-24 years are infected.
More than 1 million sexually transmitted infections (STIs) are acquired every day worldwide (1, 2).
Each year, there are an estimated 376 million new infections with 1 of 4 STIs: chlamydia, gonorrhoea, syphilis and trichomoniasis (1, 2).
More than 500 million people are estimated to have genital infection with herpes simplex virus (HSV) (3).
More than 290 million women have a human papillomavirus (HPV) infection (4).
The majority of STIs have no symptoms or only mild symptoms that may not be recognized as an STI.
STIs such as HSV type 2 and syphilis can increase the risk of HIV acquisition.
988 000 pregnant women were infected with syphilis in 2016, resulting in over 350 000 adverse birth outcomes including 200 000 stillbirths and newborn deaths (5).
In some cases, STIs can have serious reproductive health consequences beyond the immediate impact of the infection itself (e.g., infertility or mother-to-child transmission)
The Gonococcal Antimicrobial Resistance Surveillance Programme has shown high rates of quinolone resistance, increasing azithromycin resistance and emerging resistance to extended-spectrum cephalosporins. Drug resistance, especially for gonorrhoea, is a major threat to reducing the impact of STIs worldwide.
The ability of an individual to pay debt and implement successful projects determines his financial strength. Financial strength is measured using the credit report which is used to stipulate the credit worthiness of an individual. To be successful in implementing and maintenance of a viable investment, cash is required. On the other hand, when debt is decreased, credit worthiness subsequently increases making it possible for a firm or an individual to seek extra finance to take on huge projects.
Moreover, when the debt is decreased, an individual can peacefully concentrate on taking other investments or personal assets such as mortgage or vehicles that would not have been possible with the existence of the debt. Therefore, after receiving $5,000, it is advisable to lower the debt since it translates to a positive credit score in the long run.
The terms of credit and available credit are influenced by a firm’s credit score. Lenders use the credit score to determine the financial health of a firm by ordering a credit report. The report indicates the amount of risk that the bank would be taking if it sources finance to the firm. According to FICO (2015), a credit score is a summary of a firm’s or an individual’s credit risk for a specific period and it is used by lenders to assess the credit report.
The $5,000 received by the firm should be used to lower the debt for a positive credit score. Though credit rating would not increase immediately, consistent payment of the debts would lead to a rise of the score. Investing is risky especially when returns are not guaranteed plus the cash was received unexpectedly, so there hadn’t been any plans to facilitate successful investment.
The autism society of community is based in the state of Los Angeles. It is also referred to as ASLA and it deals with taking care of the autism children living within the larger community of Los Angeles (Koegel et al., 2013). Autism Spectrum Disorder (ASD) (2013) asserts that the autism community has an overall aim of ensuring they have made a major differences in the lives of the people living with the autism conditions.
Furthermore, the families of the children suffering from autism make use of the services being provided by the community. The autism community has also employed a lot of health care professionals who take care of the children suffering from mental challenge.
The autism community was created in the year 1965 (Koegel et al., 2013). It was created when the abnormality condition was not highly known among the community members. It is considered one of the oldest, as well as the largest, in terms of taking grass root measures in Los Angeles. It has over 45 years of expertise in taking care of the autism children (Autism Spectrum Disorder (ASD), 2013).
This is due to the fact that it provides a lot of information concerning people suffering from autism while at the same time carrying out adequate research concerning the issue. The total number of members of ASLA community exceeds 120,000 where the supporters have remained connected in a very functional network system (Koegel et al., 2013). According to Koegel et al. (2013), they are connected in over 150 chapters in the whole of Los Angeles.
Thu, the community has also come up with objectives. First, it aims at raising money, both locally and in outside organizations, in order to cater for the demands made by the people suffering from autism. Secondly, ASLA has also been able to bring together the professionals, the interested individuals, the supporters, and the collaborators of the community in order to take care of the needs and requirements of the children suffering from autism.
Community Partnership of the Autism Society of Los Angeles
And Additional Partnership Deemed Important
The Autism Society of Los Angeles has also formed multifaceted partnerships with several important organizations to strengthen its overall operations. The formation of good partnerships has been one of the key pillars that has bolstered the process of effective delivery of the services.
The autism community group has enabled the formation of a very strong bond between the Autism Society National Society and it. Koegel et al. (2013) avers that the major aim of formation of such a partnership is to ensure there is formation of a strong bond between the organization and other related local organization in other parts of the United States.
Apart from that, it has also been able to form strong partnership with other important stakeholders and figures such as the leaders, parents, and the key professionals (Autism Spectrum Disorder (ASD),2013). ASLA is very much aware that the formation of strong bond between it and the parents of children suffering from autism acts a very important stepping stone in building a strong bond in enhancing the process of services delivery.
The whole process has helped the parents to develop trust and confidence with the operations being carried out by ASLA, thus, acting as an important facilitator in compelling the parents to entrust it with the taking care of their children.
Contrarily, the professionals have also collaborated with the autism community in order to improve the process of service delivery. For instance, the special educationists have been able to access a chance for addressing important issues they would like to see addressed in order to improve the experience autism children gain over the time they spend in ASLA (Becerra et al., 2012).
Moreover, some professionals have also volunteered to offer some of the skills they deem important in trying to improve the lives of the autism children. The local leaders in Los Angeles have also passed beneficial laws that have favored the activities and operations of ASLA. The major aim of passing such laws and amendments is to make sure the children suffering from autism attains optimal support from the government (Hanney et al., 2012).
The leaders have also developed important financial kitties in order to fund important autism programs (Autism Spectrum Disorder (ASD), 2013). Unlike the normal children, those suffering requires special treatment when being educate. As a result, the local authorities have moved in to support ASLA by closing the financial gap for the effective delivery of its services while at the same time meeting its overall objectives.
Nonetheless, the organization can improve its operations by making sure it has formed more partnership with other significant parties. For instance, it should seek forming partnership with significant parties such as the global autism societies (Autism Spectrum Disorder (ASD), 2013).
The move will help incorporate ideas that have far-reaching improvements towards the lives of children suffering from autism. ASLA can also form strong partnership with religious affiliated groups (Becerra et al., 2012). This is due to the fact that such groups are more likely to offer positive contributions towards the lives of the autism children. It can also partner with more charitable organizations in order to expand its educational kitty.
The Cross-Cultural Challenges and the Humanitarian Considerations Enshrined In ASLA
The team of the professional plays a very important role in trying to determine the major decisions made by ASLA during the implementation of the major changes. The pool of professionals have recommended that the autism community should embrace the multicultural system in operating most of its affairs. They understand that the majorities holds different reasons concerning why children suffer from autism.
These may range from mode of vaccination, illnesses, environmental, perennial factors, and the hereditary. Therefore, they have helped to bring all these cross-cultural issues on board in order to come up with a comprehensive system for helping children suffering from the autism condition (Autism Spectrum Disorder (ASD), 2013). The parents have also a very important role especially when it comes to the suggestion of the ways their children should be treated and diagnosed (Becerra et al., 2012).
As such, most of the policies used to govern the operations of ASLA depends on the cultural background regarding the different families that are of interest in the autism community (Becerra et al., 2012). This is due to the fact that the decisions they make are influenced by several cultural factors such as the primary language used, the rituals, the beliefs, the values, the religious backgrounds, and the traditions of the parents.
Despite the incorporation of the cross-cultural set up or issues, there is still scanty availability of information concerning the application of the origin of the autism in children. Thus, there is need for ASLA to listen to the reasons being offered by both parents and the professionals as the main reasons for the occurrence of autism in children.
The move helps to offer an important background for the application of the appropriate remedies during the initiation of intervention procedures (Autism Spectrum Disorder (ASD), 2013). For example, children from different cultural backgrounds may have varying length of delayed embracement of their respective languages (Williams et al., 2013). While the trend may seem to be normal, there is need to incorporate important ideas concerning autism in order to determine how appropriate remedies can be applied.
The proposal for such remedies should be the sole purpose of the professionals and the care takers living within the community. Therefore, they would be able to understand how to apply the appropriate remedies based on the cultural setup of the different communities and religious groups living in Los Angeles.
The Autism Society of Los Angeles and how it makes Use of the Economic Benefits Associated with It
The autism community has a lot of economic benefits it can take advantage of to improve the overall delivery of its services towards the children suffering from the mental challenge. The autism community has put it clear that anybody can feel free to offer any form of financial assistance in its official website pages (Hanney et al., 2012). As a result, the move has helped it register tremendous improvements in terms of the bulging of funds kitty.
As a result, ASLA has managed to buy equipment meant for the facilitation of better education for the children suffering from the autism condition (Williams et al., 2013). Apart from that, the autism community has also welcomed volunteers who are interested in working and uplifting the lives of the children suffering from autism (Ennis-Cole et al., 2013). The volunteers have been at the forefront in trying to make sure the autism children are able to learn how to carry out basic events in life such as cleaning of the environment and rehabilitating the environment (Williams et al., 2013).
The larger Los Angeles community is also allowed to visit and entertain the autism children during the major events or days such as the Family Fun Day and other religious holidays such as the Easter Festive (Ennis-Cole et al., 2013). During such events, the children are encouraged to compete in activities such as the painting, mowing grass, and playing in order to create a strong competitive edge among themselves (Hare, 2012). Therefore, they are able to keep on improving their overall mental capability.
Basic Hindrances the Autism Society of Los Angeles Faces When Trying To Look For the Effective Remedies
There is strong belief that autism, among the children, is a sign of curse in respective families. As a result, the strong cultural beliefs has made the treatment and fully embracement of the children suffering from autism a serious challenge (Laugeson et al., 2015). There has been cases where some parents have declined taking their children to the facility in order to access the special needs sighting issues such as curse (Laugeson et al., 2015).
Thus, it is upon ASLA to come up with more appropriate remedies that can create awareness among the parents of such children to embrace the abnormality just like any other. In fact, it should create more open ways of communication in order to promote open sharing of information regarding autism, where some families considered the issues as a taboo (Hanney et al., 2012). This would help erase the anxiety that might be associated with the autism condition among the children in Los Angeles.
In the long run, the launching of a strong campaign, which promotes a strong awareness about the mental condition will help to erase the frustration that might be associated with the parents seeking help (Hare, 2012). The move will promote the development of an open rapport. Some of the therapeutic procedures, which should be encouraged include the embracement of the Positive Behavior Support and the Discrete Trial Training. These will be very important policies that will help to promote the development of a positive feedback concerning the matter.
Vision of the Autism Society of Los Angeles
ASLA has created its vision it would like to see being achieved in the future. The community aims at promoting and facilitating the autism children towards realizing their full potential especially within the Los Angeles State (Special Education Needs, 2013).The major aim of promoting the positive realization of their full potential is to enable them grow into fully responsible citizen, who are able to think independently and have a positive impact towards the rest of the society just like the normal children.
The Proposed Improvement and the Important Changes the Autism Society of Los Angeles Should Make
The organization will need to come up with more appropriate measures that will seek at discrediting the fact that autism children signals a curse towards the respective families. In fact, this is the only way there will be dislodging of such claims (Sun et al., 2015). The community should also mount string campaign network through the social media trying to promote need for being open enough in about the autism in children (Sun et al., 2015).
Feasible Contributions One Can Make towards the Organization’s Activities
There are different ways that one can participate towards improving service delivery in ASLA community. One can become a volunteer where he/she can take the autism children through important life tasks in order to promote their independent thinking such as encouraging them to embrace graphic designs (Sun et al., 2015).
Moreover, it will also be important in trying to promote the funding process of the organization where one can remain very active in looking for donations. Moreover, regular broadcasting and communication process and important progresses being made by ASLA is also another important opportunity a person can seek at participating in, thus, promoting the creation of more awareness.
Sun, X., Allison, C., Matthews, F. E., Zhang, Z., Auyeung, B., Baron-Cohen, S., & Brayne, C. (2015). Exploring the Under-diagnosis and Prevalence of Autism Spectrum Conditions in Beijing. Autism Research, 8(3), 250-260. Retrieved from http://onlinelibrary.wiley.com/doi/10.1002/aur.1441/pdf
Delegation in Nursing refers to assigning of nursing duties to a junior nursing staff or an individual who has not undergone nursing training. It is an important aspect of nursing since it enables patients to receive healthcare services any time they are required. It is important to note that the delegating nurse remains accountable for the activities delegated. Consequently, they are as well responsible for the activities they delegate (Berman et al. 2012).
In delegation in nursing, there are some factors which the registered nurse should factor out. They are referred to as the rights of delegation. To begin with, the should assess a situation and make a decision on which activity can be delegated to another individual, that is, the right task for the right patient (Dalton & Levett-Jones, 2015). The task to be delegated depends on the staff’s level of competency and availability of supervision.
Therefore, the registered nurse should make judgment on the level of supervision which would fit the circumstance (Cowan, Brunero, Lamont & Joyce, 2015). Also, the nurse should identify the healthcare needs to be addressed by the delegated task and what will be the outcome. Delegation in nursing has to consider Nursing ethics.
Moreover, the RN takes into account the skills and capabilities of the delegatee to be in a position to assign a given task. Finally, there should be clear communication on what, how and when a particular task should be done. It involves the purpose, the goal and limitations. Finally, it is the responsibility of the registered nurse to monitor and after that evaluate both the patient and the performance of the staff for the delegated tasks (Dalton & Levett-Jones, 2015). The RN intervenes for the patient and provides feedback so as t enhance improvement in case a similar function is given out.
According to the Nursing and Midwifery Board of Australia, a registered nurse is usually held accountable for direct supervision and delegated tasks. During a nurses period of practice, there are so many issues that come up, and she is required to analyze and think critically pertaining an issue and come up with an intervention (Nursing and Midwifery Board of Australia, 2012).
A registered nurse is also supposed to utilize delegation, supervision, and coordination to ensure the best outcome for the patients. The registered nurse delegates nursing activities to enrolled nurses and others in line with their scope of practice or any other clinical or non-clinical personnel. Also, the RN should ensure that the delegated method is safe and right through provision of proper direction and supervision.
To begin with, I would attend to the collapsed post-operative patient who had collapsed. This is an emergency and needs to be attended to immediately so as to offer resuscitation. Meanwhile, I would delegate to the nurse assistant to attend to Mrs. Smith visitor, and clear information would be given to her on the activities to carry out.
Also, I would delegate to the enrolled nurse to give medication to the patient awaiting cardiac catheterization. Then, the enrolled nurse and I would attend to the patient with the cannula that had tissued to ensure she receives her due medication. The registered nurse would demonstrate to the enrolled nurse on how it has done since she has a responsibility to teach her colleagues. I would then delegate the Clerk to liaise with the maintenance to attend to the blocked toilet
Finally, I would go to discuss the medication error that had occurred the previous week with the medical consultant The Registered Nurse remains accountable for all activities that take place in her unit (Berman et al. 2012). It is, therefore, to follow the rights of delegation so as to ensure best patient care outcomes. Finally, the enrolled nurse would be requested to administer medication to the patient before It is important to note that, after delegation, a registered nurse should accept accountability for decisions actions and responsibilities for the actions of the others whom she has delegated responsibilities.
References
Berman, A., Snyder, S.J., Kozier, B., Erb, G., Levett-Jones T., Dwyer, T., Hales, M., Harvey, N., & Stanley, D. (2012). Kozier and erb’s fundamentals of nursing (2nd ed.). Vol 2, NSW: Pearson Sydney Australia.
Cowan, D., Brunero, S., Lamont, S., & Joyce, M. (2015). Direct care activities for assistants in nursing in inpatient mental health settings in Australia: A modified Delphi study. Collegian, 22(1), 53-60.
Cowen, P. S., & Moorhead, S. (2014). Current issues in nursing. Elsevier Health Sciences.
Dalton, L., Gee, T., & Levett-Jones, T. (2015). Using clinical reasoning and simulation-based education to ‘flip’the Enrolled Nurse curriculum. Australian Journal of Advanced Nursing, 33(2), 29-35.
Duffield, C., Roche, M., Twigg, D., Williams, A., & Clarke, S. (2016). A protocol to assess the impact of adding nursing support workers to ward staffing. Journal of advanced nursing.
McCarthy, G., Cornally, N., O’Mahoney, C., White, G., & Weathers, E. (2013). Emergency nurses: procedures performed and competence in practice. International Emergency Nursing, 21(1), 50-57.
Want help to write your Essay or Assignments? Click here