Parents have great influences in their children social cognition. For this reason, the eligible participants for this study include adolescents diagnosed with Autistic Spectrum Disorder (ASD), age 16- 23 years and together with their parents or the primary caregiver (Hartley, Schaidle, & Burnson, 2013; Loukas et al., 2015). The inclusion criteria for participants included the ability to communicate in English, and the adolescent is diagnosed with ASD.
Participant recruitment will take place at the community clinical settings. Emails requesting for participation will be sent to the adolescent’s parents/ caregivers diagnosed with ASD. The email will include the project’s description in detail, including the benefits and risks associated with their participation. The parents who are interested in participating will be requested respond to the email and will be contacted for official recruitment processes including the signing of the informed consent
Sample collection is an integral part of research design as it determines whether the research hypothesis will be appropriately tested. Therefore, it is important to establish a balance between an ideal sample and a convenient (Kandalaft et al., 2013). At the commencement of the study, the available study sample is estimated at ten pairs of participants, that is ten adolescents diagnosed with ASD and ten parents/caregivers of the adolescents diagnosed with ASD. However, due to unavoidable circumstances, the study sample may slightly less than the estimated number.
The study sample will be pretested using questionnaires to evaluate the adolescent’s social cognition ability at the baseline. This will be followed by the proposed intervention (training for adolescents and their parents for 15 weeks). After 15 weeks, a post-test and a focus group discussion will be performed to determine the impact of the intervention and to understand the challenges adolescent’s experiences during the transition.
References
Hartley, S. L., Schaidle, E. M., & Burnson, C. F. (2013). Parental Attributions for the Behavior Problems of Children and Adolescents With Autism Spectrum Disorders. Journal of Developmental and Behavioral Pediatrics : JDBP, 34(9), 651–660. http://doi.org/10.1097/01.DBP.0000437725.39459.a0
Kandalaft, M. R., Didehbani, N., Krawczyk, D. C., Allen, T. T., & Chapman, S. B. (2013). Virtual Reality Social Cognition Training for Young Adults with High-Functioning Autism. Journal of Autism and Developmental Disorders, 43(1), 34–44. http://doi.org/10.1007/s10803-012-1544-6
Loukas, K. M., Raymond, L., Perron, A. R., McHarg, L. A., & LaCroix Doe, T. C. (2015). Occupational transformation: Parental influence and social cognition of young adults with autism. Work, 50(3), 457-463.
Want help to write your Essay or Assignments? Click here
DIFFERENCE BETWEEN HISTORICAL AND CONTEMPORARY MENTAL HEALTH CARE
INTRODUCTION
Mental health care practice began several years ago when relatively simple approaches to care were still being utilized. Like any other form of health care, mental health care can be evaluated based on a range of theories and models which have extensively been used to inform mental health nursing practice. This paper discusses the difference between historical and contemporary mental health care as it applies to nursing models and the nursing process.
This paper has described in details, the concepts of “nursing process” and “nursing model” and how they have evolved since conception. Moreover, this paper uses a case study to describe how the nursing process and a nursing model have been applied in nursing care provision for a patient who is suffering from a sexually transmitted infection characterized by depression.
CONTEMPORARY AND HISTORICAL MENTAL HEALTH CARE
2.1 The Nursing Process and how it has Evolved since Conception
The principles of nursing process largely dominate mental health care practice in today’s nursing and health industry. The term “nursing process” is defined as the application of a scientific approach to care provision that involves strict adherence to distinct steps which are aimed at generating positive health outcomes for patients (Perez-Rivas, Martin-Iqlesias, Pacheco del Cerro, Arenas, Lopez and Lagos, 2016, p. 43).
According to Perez-Rivas et. al., (2016, p. 43), for a nursing process to be considered effective, the health care practitioner must complete all the documented steps because information gained from one step results into the success of subsequent steps. Approaching mental health care based on the principles of “nursing process” helps to develop critical thinking skills of nurses, which eventually translates into improved problem-solving and positive health outcomes for mentally-ill patients (Perez-Rivas et. al., 2016, p. 44).
Nursing process and its application in mental health care has greatly evolved from when it was introduced up to date. Traditionally, the nursing process extensively emphasized on health care assessment, implementation of intervention, and planning as the only phases involved in mental health care delivery. In those days, the process did not recognize the significant role played by cognitive processes in influencing decision making during care (Zamanzadeh et. al., 2015, p. 411).
However, as nurses continued to utilize the historical principles of the nursing process into practice, increasingly advanced nursing processes were integrated and this has greatly improved the overall image of the nursing process. For instance, the advanced nursing process currently integrates diagnostic reasoning that facilitates decision making which was absent in the traditional nursing process.
Through continued nursing research and practice, nursing professionals have contributed greatly to the evolution of the nursing process by identifying the need to incorporate health outcomes identification and planning into the nursing process. To date, health care professionals who handle mental health cases view the nursing process as an advanced form or practice that involves five steps: “assessment, diagnosis, outcome identification and planning, intervention implementation, and evaluation (Zamanzadeh et. al., 2015, p. 412).
2.2 How the Nursing Process was First Developed and How it is used in Contemporary Nursing
The nursing process that is used in contemporary nursing differs significantly from the one used in traditional nursing as it applies to mental health care. This is attributed to the changes that have been made on the “nursing process” since it was developed (Perez-Rivas et. al., 2016, p. 44). Nursing was first viewed as a process rather than a distinct activity in 1955 by Lydia Hall from United Kingdom.
Although many professionals in the nursing field were not sure as to whether Hall’s views were right, a few of them dwelled extensively on the topic and they began to refer to nursing as a process. Examples of authors who supported Hull in describing nursing as a process include Johnson, Orlando, and Wiedenbach and their opinions on the nursing process are available in their publications of 1959, 1961, and 1963 respectively.
By then, only three steps were used to define the nursing process and they include, “assessment, planning, and evaluation (Zamanzadeh et. al., 2015, p. 411).” These three steps provided the basis of the nursing process that traditional nurses used to deliver mental health care to patients.
Later on in 1967, an additional step described as implementation of intervention was added to the nursing process by Walsh and Yura. It is not until 1973 when the American Nurses Association (ANA) felt in necessary to incorporate diagnosis into the nursing process. During the final revision and publication of the ANA standards in 1991, another step known as identification of outcome was integrated into the nursing process.
The step was made part of the planning phase and this resulted into the generation of a nursing process that comprised of five steps namely; “assessment, diagnosis, outcome identification and planning, intervention implementation, and evaluation (Zamanzadeh et. al., 2015, p. 412).” The development of the nursing process has progressed through a number of steps which have been modified across years to generate the process that is currently used in contemporary nursing to provide care for mentally-ill patients.
Based on the nursing process, contemporary nurses frequently assess, diagnose, identity outcomes, implement interventions, and finally evaluate the effectiveness of interventions whenever they are delivering mental health care to patients.
2.3 The Nursing Model and How they Have Evolved Since Conception
Nursing models play a very important role in nursing practice in the sense that, they largely influence decision making processes by nurses concerning the most appropriate ways through which patients should be handled. A nursing model is defined as a framework of nursing concepts that act as a foundation for nursing care and that describe how given health care practices should be performed (Murphy, Williams and Pridmore, 2010, p. 23).
Nursing models have been developed to help direct nurses on the best approaches they should take to improve patient outcomes and to explain why certain approaches as relevant. Different nursing models exist and their goal is to assist nurses to achieve various nursing components based on the nature of a mental health issue they are handling at any given time (Springer and Casey-Lockyer, 2016, p. 647).
Nursing models have significantly evolved since their conception due to constant changes in patients’ needs and due to rapid technological advancements in the contemporary world which tend to change approaches to care. Nursing models were first developed in the United States way back in 1960s (Murphy, Williams and Pridmore, 2010, p. 23). In 1960, the United States was characterized by a number of cultural, technological and social transformations which influenced nursing professionals to make changes that were aimed at improving nursing practice.
For this reason, traditional nursing models were developed based on their effectiveness in meeting basic medical goals. For instance, the “medical model” provided a foundation only for the management of physical health problems. Nurses in the United Kingdom began to apply nursing models into practice in 1970s (Murphy, Williams and Pridmore, 2010, p. 24).
Since then, significant transformations in the world have helped nurses to build a body of knowledge that has been used to develop modern nursing models. Nursing models which are used in contemporary nursing to deliver mental health care have been developed to guide nurses on how they can handle patients with a wide variety of health problems as opposed to traditional models (Springer and Casey-Lockyer, 2016, p. 660).
2.4 Total Patient Care: A Historical Nursing Model
An example of a historical nursing model that is rarely used by today’s nurses is Total Patient Care which is also known as Private Duty Nurses. Total Patient Care is a nursing model that conceptualizes that, for nurses to deliver quality patient care, they must have a small number of patients that they can effectively handle at any given time. The nurse should then work in collaboration with other registered nurses to ensure that the patients being attended to receive maximum care.
Total Patient Care model guided traditional nurses to work with small groups of mentally-ill patients that they could effectively handle at any given time. Although Total Patient Care can still be used to guide clinical decisions in today’s health care settings, today’s health care organizations rarely utilize this model to deliver mental health care (Mary and Sandra, 2004, p. 291).
2.5 Watson’s Theory of Caring: A Contemporary Nursing Model
Through his theory of caring, Jean Watson greatly influences clinical decision making processes by today’s nurses, especially those who deliver care to patients with mental health problems. This contemporary nursing theory conceptualizes that there are four major factors that determine positive patient outcome during care delivery. These factors include the personality of the care giver, the patient’s health status, the environment in which care is delivered, and the nursing process (Ozan, Okumus and Aytekin, 2015, p. 26).
These factors influenced Watson to assume that the most effective form of care is that which is delivered interpersonally. In addition, the nurse should take time to understand specific health problem that a patient is suffering from. Again, it is the responsibility of the nurse to create caring environment for his or her patient. Furthermore, nursing lies at the center of caring and intended health outcomes will only be achieved if the right nursing processes are followed. Watson’s theory of caring is widely used in nursing practice today (Ozan, Okumus and Aytekin, 2015, p. 25).
SERVICE USER’S HISTORY
A service user whom I have cared for in the past is a female patient aged 16 years and who suspected that she was suffering from a sexually transmitted infection and was therefore in need of medical care. I had to take historical data before I could identify the best component of the nursing process to use in order to confirm presence or absence of a sexually transmitted infection.
My patient was an orphan who stayed with her uncle at the time of visit. At the time of visit, she was feeling depressed and psychologically disturbed because of her health condition. In addition, she was part of a group of commercial sex workers in the city despite her young age, and she uses money earned from the business to earn a living. She had also been in an intimate relation with different partners without protection.
Her uncle used to beat her up every time he was at home and therefore, she feared staying at home. The patient had not taken any medication prior to visiting the health care facility. I applied the nursing process to deliver the most appropriate nursing care for the patient.
When I was handling my patient, I greatly relied on the nursing process that is majorly used in contemporary nursing. By following the five steps of the nursing process, contemporary nurses are able to provide quality care that addresses specific patients’ needs. During assessment phase, the contemporary nurse collects, verifies, organizes, interprets, and documents patients’ health data that will be used to accomplish the subsequent steps.
After collecting relevant data, the contemporary nurse ensues to diagnosis phase where he or she analyzes the collected data to make a clinical judgment which is aimed at identifying a specific health problem that the patient is suffering from (Perez-Rivas et. al., 2016, p. 44).
Once a specific health problem is identified, the contemporary nurse proceeds to the third phase where he or she identifies the most appropriate health outcomes that the patient should be assisted to achieve. It is in this phase where the nurse documents a plan of how the patient can be helped to achieve the proposed outcomes. In the fourth phase, the contemporary nurse implements the right intervention as documented in the plan (Zamanzadeh et. al., 2015, p. 416).
The nurse then proceeds to the fifth phase where he or she evaluates the effectiveness of the implemented intervention in generating the proposed health outcomes for the patient. In case the proposed health outcomes are not realized following intervention implementation, the nurse is compelled to change the intervention until the intended results are obtained (Perez-Rivas et. al., 2016, p. 44).
A component of the nursing process that I used to exercise care for the patient was taken from the Assessment, Diagnosis, Planning, Implementation, and Evaluation (ADPIE) model described above, considering the fact that it is the one that is widely used in contemporary nursing. I decided to use Diagnosis component of the ADPIE to maximize nursing care for my patient.
By choosing diagnosis component, I wanted to bring together all the historical data that I had gathered into meaningful information. Specifically, when conducting diagnosis on the patient, I used the data that I had already collected to make clinical judgment about my patient and the family. This enabled me to understand that risk factors that exposed by patient to acquiring sexually transmitted infections.
Furthermore, I was able to predict possible responses that she could receive from family members if she approached them with her health problem. Generally, diagnosis provided me with the basis for selecting the most appropriate nursing intervention that could generate positive health outcomes for my patient.
The type of diagnosis that I conducted on the patient was possible nursing diagnosis. A possible nursing diagnosis is conducted when a patient’s problem requires additional analysis for the presence or absence of a health problem to be confirmed (Perez-Rivas et. al., 2016, p. 44). In the case that I was handling, it was not yet confirmed that the patient was suffering from sexually transmitted infections. The client was worried that she might have acquired sexually transmitted infections owing to her sexual behaviours in the recent past. Such thoughts had severe impact on her mental health. Data obtained from this diagnosis helped me to confirm presence of a sexually transmitted infection (Zamanzadeh et. al., 2015, p. 416).
Diagnosis was a very important component of ADPIE for my patient because it acted as a link to the other aspects of the nursing process namely; planning, implementation, and evaluation. The diagnosis was the second phase of the nursing process that was performed after collecting data in the assessment phase. Information gathered during diagnosis phase was extremely useful in the subsequent steps because I utilized it to identify the best health outcomes for my patient and to select a nursing intervention that could generate those outcomes for my patients. Diagnosis was very important in the overall nursing process because it helped me to come up with the right interventions that were intended to generate improved health outcomes for the patient (Zamanzadeh et. al., 2015, p. 416).
When I was providing nursing care to my patient, I paid greatest attention to Watson’s Theory of Caring mode. I utilized the four major factors that determine positive patient outcome during care delivery as described in Watson’s theory of caring. Specifically, I strived to; build strong interpersonal relationship with the client, establish specific health problem the patient was suffering prove, create an environment suitable for nursing care, and to adhere to all steps of the nursing process (Ozan, Okumus and Aytekin, 2015, p. 25).
CONCLUSION
Historical and contemporary mental health care differ significantly due to evolutions in nursing theories and models which have taken place over the years. For instance, while traditional mental health care was delivered using a nursing process that only involved three steps, delivery of contemporary mental care utilizes a nursing process with five steps.
Additionally, while traditional mental health care was based on historical nursing models, today’s mental health care is guided by contemporary nursing models such as Watson’s theory of caring model. The evolutions of the nursing process and the developments of nursing models have brought about significant improvements in health care delivery particularly in mental health care.
From this case study, I have learnt the importance of implementing contemporary nursing processes and nursing models in care delivery. I will utilize this knowledge to improve the quality of mental health care that I will deliver in future. As a student nurse, I will take my time to evaluate and understand changes in nursing models and components of the nursing process as they apply to mental health care.
References
Mary, T. & Sandra, L. 2004, “Traditional models of care delivery: What have we learned?” Journal of Nursing Administration, vol. 34, issue 6, pp 291-297.
Murphy, N., Williams, A. & Pridmore, J. A. 2010, “Nursing models and contemporary nursing 1: The development, uses and limitations,” Nursing Times, vol. 1, issue 106, p. 23-24.
Ozan, Y., Okumus, H., & Aytekin, A. 2015, “Implementation of Watson’s theory of human caring: A case study,” International Journal of Caring Sciences, vol. 8, issue 1, pp. 25-35.
Perez-Rivas, F., Martin-Iqlesias, S., Pacheco del Cerro, K., Arenas, C., Lopez, M. & Lagos, M. B. 2016 “Effectiveness of nursing process use in primary care,” International Journal of Nursing Knowledge, vol. 27, no. 1, pp. 43-47.
Springer, J. & Casey-Lockyer, M. 2016, “Evolution of a nursing model for identifying client needs in a disaster shelter: A case study with the American Red Cross,” Nursing Clinics of North America, vol. 15, no. 4, pp. 647-662.
Zamanzadeh, V., Valizadeh, L., Tabrizi, F., Behshid, M. & Lotfi, M. 2015 “Challenges associated with the implementation of the nursing process: A systematic review,” Irarian Journal of Midewifery Research, vol. 20, no. 4, pp. 411-419.
Want help to write your Essay or Assignments? Click here.
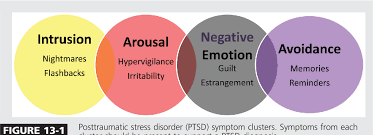
Many people tend to develop Post Traumatic Stress Disorder, (PTSD), after witnessing a life threatening events such as terrorism, road accidents, veteran wars, fire accidents, as well as natural disasters such as earthquakes and floods. While treatment approaches have always been used to help individuals to recover from PTSD symptoms cluster: re-experiencing, avoidance/numbing, and hyper arousal, major aspects of spirituality can also be applied to promote recovery.
In this regard, both Christian counseling and clinical group therapy can help to eliminate the PTSD symptoms cluster: re-experiencing, avoidance/numbing, and hyper arousal. Ideally, Christian counseling and clinical counseling are intended to achieve a common goal about five major areas including; duration of treatment, the relevance of truth, the role of a community of support, possession of faith and motivation to persevere, as well as the role played by acceptance and hope in healing.
Following severe traumatic events, victims commonly present with psychological changes that occur as they try to recall either what they saw or felt during the event. These psychological reactions may lessen if proper counseling interventions are applied immediately after the traumatic event. However, if not managed quickly, individuals may suffer constant mental problems accompanied by emotional distress, a condition that is often referred to as post-traumatic stress disorder (PTSD) (Sareen, 2014).
Sareen (2014) defines PTSD as a mental disorder that occurs as a result of either witnessing or directly experiencing a life-threatening event. With the rapid rise in traumatic events such as terrorism, road accidents, veteran wars, fire accidents, as well as natural disasters such as earthquakes and floods, PTSD is becoming a health concern in the society that needs to be addressed with a lot of commitment.
Effective interventions should be implemented to help prevent serious health problems that may occur from PTSD symptoms cluster: re-experiencing, avoidance/numbing, and hyper arousal (Cohen and Scheeringa, 2009; & Wilkins, Lang, and Norman, 2011).
Effective elimination of PTSD symptom cluster requires a combination of, psychological, spiritual, and pharmacological approaches to treatment (Walker, Scheidegger, End, and Amundsen, 2012). The thesis statement that guides current research states that group therapy intervention for managing PTSD symptoms cluster: re-experiencing, avoidance/numbing, and hyper arousal, is based on significant aspects of spirituality.
The purpose of this research is to explore the major aspects of spirituality that are related to group therapy management for PTSD symptoms cluster: re-experiencing, avoidance/numbing, and hyper arousal, while citing teachings of the Bible as well as information obtained from some theoretical resources.
Before analyzing the significant aspects of spirituality that are related to PTSD symptoms cluster, it is important to understand the specific symptoms that a clinical psychologist and a Christian counselor intend to help their clients to recover from. In the fourth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV-TR (1), the American Psychiatric Association has documented specific symptoms that clinicians should substantiate during PTSD diagnosis.
According to the American Psychiatric Association’s DSM-IV, PTSD should be diagnosed based on three symptoms cluster namely; re-experiencing, avoidance/numbing, and hyper arousal (Goldstein, Bradley, Ressler and Powers, 2017, p. 319). As far as re-experiencing criterion is concerned, people with PTSD individual persistently recall what was either felt or observed during a traumatic event. To prove that a client regularly recalls the happenings of the traumatic event, he or she must present with at least one of the documented five ways.
The five documented presentations include; repeated and disturbing recollection of the happenings of the traumatic event accompanied by perceptions, images, and thoughts; repeated disturbing dreams related to the event; behaving as if the traumatic event was happening again; severe psychological disturbance whenever one comes across issues that look like the life threatening event; and physiologic disturbance any time an individual comes across things that resemble the life threatening event.
As Kleim, Graham, Bryant, and Ehers (2013) explain, it has been discovered that survivors of traumatic events have a tendency of constantly recalling those happenings, and that people often react differently depending on the degree of psychological impact that they have faced from those events.
Concerning avoidance/numbing criterion, an individual who is suffering from PTSD is believed to have a tendency of constantly escaping from stimuli that are related to the distressing event. Furthermore, these people often become less responsive to activities accompanied with feelings of isolation, which did not occur before the life-threatening event.
An individual must demonstrate at least three of the seven behavioral characteristics that have been documented in DSM-IV regarding PTSD diagnosis. The seven features that have been documented by the American Psychiatric Association include; struggling to avoid perceptions, discussions, or feelings associated with the life threatening event, struggling to keep off people, places, or activities that might remind them of the traumatic event, loss of memory of the crucial aspects of the event, lack of interest in taking part in activities, feeling of isolation, inability to have feelings of affection, and loss of hope to plan for the future.
Several studies have been conducted to confirm the presence of avoidance/numbing characteristics among populations with PTSD. For instance, Naifeh, Tull and Gratz (2012) have found that persistent emotional avoidance is a common problem among patients with severe PTSD.
As far as hyper-arousal is concerned, individuals who suffer from PTSD often exhibit constant symptoms of excitement, which did not exist before the occurrence of a distressing event. For hyper-arousal to be confirmed in an individual, one must present with at least two of the documented characteristic behaviors. These signs include sleep problems, aggressiveness, extreme alertness, lack of concentration, and extremely astound response. As Weston (2014) explains, of the three signs that form PTSD symptoms cluster, hyper-arousal is the most predominant and that should be eliminated first.
As they interact with people with PTSD, both the clinical psychologist and the Christian counselor often utilize approaches which are aimed at eliminating PTSD symptoms cluster: re-experiencing, avoidance/numbing, and hyper arousal (Walker et al., 2012). Although the Bible does not give any information concerning PTSD symptoms cluster, Christian counselors often rely on biblical teachings to help individuals to recover from symptoms of PTSD.
Specifically, a clinical psychologist will utilize group dynamics to help their clients to recover from PTSD cluster symptoms, while a Christian counselor will rely on the teachings of the Bible to promote healing for PTSD clients. The use of group dynamics by a clinical psychologist to help eliminate PTSD symptoms cluster: re-experiencing, avoidance/numbing, and hyper arousal, is based on some major aspects of spirituality (Walker et al., 2012).
Both the clinical therapist and the Christian counselor strive to help individuals with PTSD to recover from re-experiencing, avoidance/numbing, and hyper arousal symptoms by encouraging them that gaining healthy functioning is a process that will take time. The Christian counselor compares the recovery process to Paul’s teachings in the Bible. In 2nd Corinthians Chapter 12, from verse 7 to verse 10, Paul has written about “thorn in the flesh” (The New King James Version).
Paul says that God provides healing at a time when He feels appropriate. He further asserts that, during times of painful experiences, God provides the suffering with enough grace to help them bear difficult situations. The Christian counselor compares re-experiencing, avoidance/numbing, and hyper arousal symptoms to the pain of a thorn. By using Paul’s teachings, an individual with PTSD gets to understand the need to be patient and develops a motivation to continue attending counseling sessions repeatedly.
In Lamentations Chapter 3, and in 1st Corinthians Chapter 1, verse 4 to 9, the Bible says that those who are in suffering should continue to present their problems to God because He is always faithful (The New King James Version). A Christian counselor uses these biblical teachings to help people with PTSD to see the need of remaining focused on the spiritual aspect of recovery.
Like spiritual counseling, group therapy by a psychologist emphasizes the need to be patient if recovery from re-experiencing, avoidance/numbing, and hyper arousal symptoms is to be realized. In psych educational group intervention, the group therapist often encourages individuals with PTSD that recovering from the three symptoms is a process that will take time. For this reason, the therapist always plans to use sessions that are extended over a given period.
This requires the group members to meet on a daily or weekly basis over some time before the three symptoms can be eliminated (Bahredar, Farid, Ghanizadeh, and Birashk, 2014). According to Substance Abuse and Mental Health Services Administration (2014), people who are exposed to traumatic events are likely to experience various impacts based on the nature and degree of the life-threatening situation.
For this reason, a group therapist must take the time to understand individual characteristics as well as the degree of psychological impact that has been created by a traumatic event for him or her to be able to help clients to recover from re-experiencing avoidance/numbing, and hyper arousal symptoms. This will require repeated interactions between the therapist and the affected individuals who will take some time (Bahredar et al. (2014).
When handling clients with PTSD symptoms cluster: re-experiencing, avoidance/numbing, and hyper arousal, both the Christian counselor and the group therapist inform their clients that they have to tell the truth for them to be able to recover from their psychological problems. Both counselors depend on the true information provided by their clients to develop and implement the best intervention for recovery (Walker et al., 2012).
During spiritual counseling sessions, the Christian counselor reminds clients with PTSD that God is always loving, and since He sees value in His people, He is always ready to forgive everyone irrespective of the nature and degree of sins they have committed (1 John 1:8–9, The New King James Version).
Also, the Christian counselor informs his or her clients that the most important thing that they should consider when evaluating their deeds is to know what God says about them but not what others speak of them. Therefore, instead of viewing themselves as either perpetrators or victims, they should identify themselves as beloved children of God as documented in Ephesians Chapter 1, verse 3 to 6, Romans Chapter 8, verse 14 to 17, and in 1st John Chapter 3, verse 1-3 (The New King James Version).
For those people who have lost their relatives and loved ones as a result of a traumatic event, the Christian counselor encourages them that God has a purpose for everyone’s life and that He protects His people by the power of the Holy Spirit (Ephesians 1:13-14, The New King James Version). By having a feeling that God loves, values, and forgives, clients can recover quickly from PTSD symptoms cluster: re-experiencing, avoidance/numbing, and hyper arousal (Walker et al., 2012).
Like it is with spiritual counseling, a group therapist in clinical counseling relies on the true statements provided by every group member to establish the most appropriate intervention plans for them (Scott et al., 2016). Ideally, for a group therapy session to be effective in eliminating re-experiencing, avoidance/numbing, and hyper arousal symptoms, clients must identify as either victim of executors of traumatic events.
Furthermore, clients must speak the truth of the specific problem behaviors that they experience as this information helps the therapist to distinguish whether the PTSD symptoms cluster are either mild or severe. The clinical psychologist who is handling PTSD clients in group therapy sessions often formulate interventions based on the truthfulness of the information provided by group members (Asher et. al., 2015).
When handling clients with PTSD symptoms cluster: re-experiencing, avoidance/numbing, and hyper-arousal, both the Christian counselor and the group therapist have an understanding that having a community to offer support will help clients to develop a deep understanding of their problems and to perform tasks that promote recovery. The Christian counselor encourages his or her clients to feel free to disclose their problems to the therapist to receive assistance from the group members.
In Romans Chapter 8 verse 35 to 38, the Bible says that nothing can separate Christians from the love of God. Also, it is documented in Hebrews Chapter 4 verse 14 to 16 that Christians should feel free to approach God and explain their problems to Him (The New King James Version). Since God can use people’s situations for His Glory, He also has the powers to restore healthy psychological functioning in individuals who are suffering from PTSD symptoms cluster: re-experiencing, avoidance/numbing, hyper-arousal (Walker et al., 2012).
The clinical psychologist who is handling PTSD patients in groups relies on support from group members to help clients to recover from re-experiencing, avoidance/numbing, and hyper-arousal symptoms. According to Norton and Kazantzis (2016), one of the advantages of group psychotherapy is the ability to obtain support from the dynamic relationships within the groups.
For this reason, the therapist strives to formulate rules that promote group cohesion as he or she acknowledges the support that every group member is likely to bring to the group (Caqueo-Urizar, Rus-Calafell, Urzua, Escudero and Gutierrez-Maldonado, 2015). As Caqueo-Urizar (2015), point out; having a community of support when caring for people with mental problems is very important because the community helps with establishing whether clients have adhered to tasks that promote healing.
Success is achieved from Christian counseling and from clinical counseling when clients are encouraged to have faith and to demonstrate a willingness to persevere from PTSD symptoms cluster: re-experiencing, avoidance/numbing, and hyper-arousal. The Christian counselor perfectly understands that managing mental health problems associated with PTSD is a huge challenge for individuals.
For this reason, the counselor repeatedly informs individuals with PTSD that they should surrender their problems to God who is always ready to show His compassion and love to the suffering. In 2nd Corinthians Chapter 1, verse 3 to 5, Paul says that God is the Father of compassion who always comforts those in trouble (The New King James Version). By relying on this biblical teaching, Christians with PTSD should have faith in God and healing, as they should develop a motivation to share in the suffering of Christ as written by Paul (Walker et al., 2012).
Similarly, the success of group psychotherapy greatly relies on faith and perseverance. People with PTSD symptoms cluster: re-experiencing, avoidance/numbing, and hyper-arousal, should have faith that the tasks that are assigned to them by the group leader will promote healing. Also, they must be ready to face the hardships associated with the assigned tasks as their commitment to adhering to group tasks is what will determine whether they will recover from PTSD or not. Eventually, positive health outcomes are always generated through a combination of faith and motivation to persevere (Reisman, 2016).
Both Christian counseling and clinical counseling emphasize on the need to accept past occurrences and to have hope for the future. According to Wilkins, Lang, and Norman, (2011), re-experiencing occurs in people with PTSD because they have a tendency of recalling what they either saw or felt during a traumatic event.
These re-experiencing symptoms can be eliminated if clients are assisted to come to terms with experiences of a traumatic event, and this can occur if they learn to accept the past. Furthermore, people with PTSD tend to lose hope in the future and lose interest in engaging in activities that promote personal growth (Naifeh, Tull, and Gratz, 2012). Therefore, the goal of the Christian counselor, as well as the clinical group therapist is to help clients to accept the past occurrences and to have hope in the future.
The Christian counselor assists individuals with PTSD symptoms cluster: re-experiencing, avoidance/numbing, and hyper-arousal, that it is important to have Hope in God because He has the powers to provide good health. The Bible says in 1st Peter Chapter 5 verse 6 to 7 that human beings should humble themselves under the powerful hand of God so that they may be exalted at the right him (The New King James Version).
In addition, in the same verse, the Bible teaches Christians that they should cast their anxieties and troubles on God because He is caring. The Christian counselor helps clients with PTSD to understand that Jesus himself experienced traumatic events and he increasingly approached God for hope. In a similar manner, by seeking help and understand from God, they will be able to recover from the mental impacts of trauma.
Like a Christian counselor, the clinician counselor always strives to assist group members to accept past occurrences and to be hopeful that they can still acquire an improved mental health (Walker et al., 2012).
In conclusion, group therapy intervention for managing PTSD symptoms cluster: re-experiencing, avoidance/numbing, and hyper-arousal, is based on major aspects of spirituality. This paper has critically explored the major aspects of spirituality that are related to group therapy management for PTSD symptoms cluster: re-experiencing, avoidance/numbing, and hyper-arousal. Explanations about the interdependence between major aspects of spirituality and group therapy management for PTSD symptoms cluster have been provided while citing teachings of the Bible as well as information obtained from a number of theoretical resources.
Asher, L., Fekadu, A., Hanlon, C., Mideksa, G., Eatom, J., Patel, V. & De Silva, M. (2015). Development of a community-based rehabilitation intervention for people with schizophrenia in Ethiopia. PLoS One, 10(11): e0143572
Bahredar, M. J., Farid, A. S, Ghanizadeh, A. & Birashk, B. (2014). The efficacy of psycho-educational group program on medication adherence and global functioning of patients with bipolar disorder type 1. International Journal of Community Based Nursing and Midwifery, 2(1): 12-19
Caqueo-Urizar, A., Rus-Calafell, M., Urzua, A., Escudero, J. & Gutierrez-Maldonado, J. (2015). The role of family therapy in the management of schizophrenia: Challenges and solutions. Neuropsychiatric Disease and Treatment, 11: 145-151.
Cohen, J. A., & Scheeringa, M. S. (2009). Post-traumatic stress disorder diagnosis in children: Challenges and promises. Dialogues in Clinical Neuroscience, 11(1): 91-99.
Goldstein, B., Bradley, B., Ressler, K. J. & Powers, A. (2017). Associations between posttraumatic stress disorder, emotion dysregulation, and alcohol dependence symptoms among inner city females. Journal of Clinical Psychology, 73(3): 319-330.
Kleim, B., Graham, B., Bryant, R. A. & Ehers, A. (2013). Capturing intrusive re-experiencing in trauma survivor’ daily lives using ecological momentary assessment. Journal of Abnormal Psychology, 122(4): 998-1009.
Naifeh, J. A., Tull, M. T. & Gratz, K. L. (2012). Anxiety sensitivity, emotional avoidance, and PTSD symptom severity among crack/cocaine dependent patients in residential treatment. Cognitive Therapy and Research, 36(3): 247-257
Norton, P. J. & Kazantzis, N. (2016). Dynamic relationships of therapist alliance and group cohesion in trans-diagnostic group CBT for anxiety disorders. Journal of Consulting and Clinical Psychology, 84(2): 146-155.
Reisman, M. (2016). PTSD treatment for veterans: What’s working, what’s new, and what’s next. Pharmacy and Therapeutics, 41(10): 623-634.
Sareen, J. (2014). Posttraumatic stress disorder in adults: Impact, comorbidity, risk factors, and treatment. The Canadian Journal of Psychiatry, 59(9): 460-467.
Scott, D., Reid, J., Hudson, P., Martin, P., & Porter, S. (2016). Health care professionals’ experience, understanding, and perception of need of advanced cancer patients with cachexia and their families: The benefits of a dedicated clinic. BMC Palliative Care, 15:100. Doi: 10.1186/s12904-016-0171-y
Substance Abuse and Mental Health Services Administration (US). (2014). Trauma-informed care in behavioral health services. Center for Substance Abuse Treatment (US): Author
The Bible: The New King James Version
Walker, K. R., Scheidegger, T. H, End, L. & Amundsen, M. (2012). The misunderstood pastoral counselor: Knowledge and religiosity as factors affecting a client’s choice. Retrieved from https://www.counseling.org/resources/library/vistas/vistas12/Article_62.pdf
Weston, C. S. (2014). Posttraumatic stress disorder: A theoretical model of the hyper arousal subtype. Frontiers in Psychiatry, 5:37. Doi: 10.3389/fpsyt.2014.00037
Want help to write your Essay or Assignments? Click here
The Five Factor Theory
In The Five Factor Theory, Costa and McCrae recognized Eysenck’s significance in identifying extraversion and neuroticism as second-order personality characteristics, as well as in establishing the Maudsley Personality Inventory, the Eysenck Personality Inventory, and the Eysenck Personality Questionnaire as instruments for assessing these variables (McCrae & Sutin, 2018).They did, however, disagree with Eysenck on psychoticism. Initially, they proposed a separate component known as openness.
When they addressed this with Eysenck, he thought openness was the polar opposite of psychoticism, while McCrae and Costa thought the elements were considerably different. Costa and McCrae have expanded on the third element of openness, adding two new second-order factors: agreeableness and conscientiousness.Costa and McCrae collaborated to create the NEO Personality Inventory (NEO-PI) to assess neuroticism, extraversion, and openness, and then the Revised NEO-PI, which additionally assesses agreeableness and conscientiousness (Costa & McCrae, 1988).
Want help to write your Essay or Assignments? Click here
The Five Factor Theory
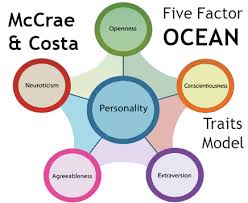
However, Paul Costa and Robert McCrae’s version is the most well-known today and the one that most psychologists think of when considering the five component model. The abbreviation OCEAN is frequently used to recall Costa and McCrae’s five components, sometimes known as the Big Five personality traits: Openness to Experience, Conscientiousness, Extraversion, Agreeableness, and Neuroticism (Costa & McCrae, 1988).
The trait of openness to experience encompasses an appreciation for art, emotion, adventure, unique ideas, curiosity, and a wide range of experiences. The degree of openness indicates a person’s intellectual curiosity, inventiveness, and appreciation for novelty and diversity. It is often referred to as a person’s level of creativity or independence. It denotes a preference for a range of activities over a tight schedule. Those with a high openness to new experiences favor novelty, whereas those with a low openness to new experiences prefer regularity (Boundless, n.d.).
Want help to write your Essay or Assignments? Click here
Conscientiousness is defined as a proclivity for self-discipline, dutifulness, competence, attentiveness, and achievement-seeking. It differs from the moral implications of conscience in that it focuses on the amount of conscious intention and thought a person puts into his or her actions (Boundless, n.d.). Individuals with a high level of conscientiousness prefer planned rather than spontaneous conduct and are frequently structured, industrious, and trustworthy.
Individuals with low conscientiousness have a more relaxed attitude, are more impulsive, and may be chaotic. Numerous studies have discovered a link between conscientiousness and academic achievement (Boundless, n.d.).
Extraversion is characterized by strong energy, pleasant emotions, talkativeness, assertiveness, friendliness, and a proclivity to seek stimulation in the presence of others (Boundless, n.d.). Low extraverts prefer alone and/or smaller groups, appreciate silence, prefer activities alone, and avoid large social situations. Because of their inquisitive and thrill-seeking character, persons who score high on both extraversion and openness are more inclined to participate in adventure and hazardous sports (Boundless, n.d.).
Agreeableness assesses a person’s proclivity to be sympathetic and helpful toward others rather than distrustful and hostile. It is also a measure of a person’s trustworthiness and helpfulness, as well as whether or not that person is typically good-tempered. People with low levels of agreeableness are often regarded as unpleasant and uncooperative (Boundless, n.d.).
Want help to write your Essay or Assignments? Click here
High neuroticism is defined by a proclivity to feel negative emotions such as wrath, anxiety, despair, or vulnerability (Boundless, n.d.). Neuroticism also refers to a person’s emotional stability and impulsive control. People with high neuroticism tend to be emotionally unstable and are described as furious, impetuous, and hostile.
They are more likely to interpret ordinary situations as threatening, and minor frustrations as hopelessly difficult (Boundless, n.d.). Their negative emotional reactions tend to persist for unusually long periods of time, which means they are often in a bad mood. These problems in emotional regulation can diminish a neurotic’s ability to think clearly, make decisions, and cope effectively with stress.
Want help to write your Essay or Assignments? Click here
Critics of the trait method say that the patterns of variability across diverse contexts are key to determining personality, and that averaging across such scenarios to find an overarching characteristic obscures important distinction between individuals (McCrae & Sutin, 2018). Critics of the Five-Factor Model, in particular, contend that it has limits as an explanatory or predictive theory and does not explain all aspects of human nature.
Some psychologists disagree with the concept because they believe it ignores other aspects of personality such as religiosity, manipulativeness, honesty, seductiveness, thriftiness, conservativeness, femininity, egotism, sense of humor, and risk-taking (McCrae & Sutin, 2018). Another common critique is that the Five-Factor Model is not founded on any underlying theory; rather, it is an empirical observation that various descriptors cluster together when factor analysis is performed. This indicates that, while these five characteristics exist, the underlying reasons are unclear.
Want help to write your Essay or Assignments? Click here
The Five Factor Theory
Trait theorists have consistently demonstrated that characteristics are extremely resistant to change once they reach maturity (Costa & McCrae, 1988). This is especially true for Neuroticism, Extraversion, and Openness, as well as for men and women, as well as for Blacks and Whites (Costa & McCrae, 1988). While Costa and McCrae recognize that people can alter drastically, consistency is definitely more essential as a general rule.
They also argue that this would be a time to be optimistic. Individuals should not be afraid of changing as they mature. If, on the other hand, a person of a younger age is lonely, sad, or suffers from another psychological ailment, they should be aware that time alone is unlikely to alter them, and that psychotherapy may be a more desired and successful course of action (Costa & McCrae, 1988).
The Five Factor Theory
Want help to write your Essay or Assignments? Click here
Costa, P. T., & McCrae, R. R. (1988). From catalog to classification: Murray’s needs and the five-factor model. Journal of Personality and Social Psychology, 258–265.
Want help to write your Essay or Assignments? Click here
Want help to write your Essay or Assignments? Click here
Five Personality Traits
Personality characteristics represent individuals’ distinctive patterns of thoughts, feelings, and behaviours. Consistency and stability are implied by personality characteristics (Cherry, 2021). Characteristic psychology is based on the concept that people differ from one another based on where they stand on a set of basic trait dimensions that endure across time and contexts. The Five-Factor Model is the five personality traits theory most often utilized trait system.
This approach comprises five basic qualities that may be recalled with the abbreviation OCEAN: openness, conscientiousness, extraversion, agreeableness, and neuroticism (Cherry, 2021). Each of the Big Five features may be subdivided into aspects to provide a more fine-grained examination of someone’s personality. Personality trait theories have long attempted to quantify the number of personality qualities that exist.
Earlier theories, such as Gordon Allport’s list of 4,000 personality traits, Raymond Cattell’s 16 personality components, and Hans Eysenck’s three-factor theory, proposed a wide range of potential qualities (Cherry, 2021). Many researchers, however, believed that Cattell’s hypothesis was too complex, and Eysenck’s was too narrow in scope. As a consequence, the five-factor theory was developed to define the basic qualities that serve as the foundation of personality (Cherry, 2021).
Want help to write your Essay or Assignments? Click here
Five Personality Traits
Openness to Experience describes a dimension of cognitive style that distinguishes imaginative, creative people from down-to-earth, conventional people (Ackerman, 2021). Open people are intellectually curious, appreciative of art, and sensitive to beauty. They tend to be, compared to closed people, more aware of their feelings. Intellectuals typically score high on Openness to Experience; consequently, this factor has also been called Culture or Intellect.
Openness is often presented as healthier or more mature by psychologists, who are often themselves open to experience. However, open and closed styles of thinking are useful in different environments (Smith, 2018). The intellectual style of the open person may serve a professor well, but research has shown that closed thinking is related to superior job performance in police work, sales, and a number of service occupations. Its facets include imagination, artistic interests, emotionality,adventurousness, intellect and liberalism.
Want help to write your Essay or Assignments? Click here
The Five Personality Traits
Conscientiousness concerns the way in which we control, regulate, and direct our impulses. Impulses are not inherently bad; occasionally time constraints require a snap decision and acting on our first impulse can be an effective response (Ackerman, 2021). Impulsive individuals can be seen by others as colourful and fun to be with. Acting on impulse can lead to trouble in a number of ways. Some impulses are antisocial. Uncontrolled antisocial acts not only harm other members of society, but also can result in retribution toward the perpetrator of such impulsive acts.
Another problem with impulsive acts is that they often produce immediate rewards but undesirable, long-term consequences (Smith, 2018). Examples include excessive socializing that leads to being fired from one’s job, hurling an insult that causes the breakup of an important relationship, or using pleasure-inducing drugs that eventually destroy one’s health.
Conscientious individuals avoid trouble and achieve high levels of success through purposeful planning and persistence (Ackerman, 2021). They are also positively regarded by others as intelligent and reliable. On the negative side, they can be compulsive perfectionists and workaholics. Furthermore, extremely conscientious individuals might be regarded as stuffy and boring. Its facets include self-efficacy, orderliness, dutifulness, achievement-Striving and cautiousness.
Want help to write your Essay or Assignments? Click here
Extraversion is marked by pronounced engagement with the external world. Extraverts enjoy being with people, are full of energy, and often experience positive emotions (Ackerman, 2021). They tend to be enthusiastic and action-oriented. In groups they like to talk, assert themselves, and draw attention to themselves. Its facets include friendliness, gregariousness, assertiveness, activity level, excitement-seeking and cheerfulness.
Agreeableness reflects individual differences in concern with cooperation and social harmony. Agreeable individuals value getting along with others. They are therefore considerate, friendly, generous, helpful, and willing to compromise their interests with others’ (Ackerman, 2021). Agreeable people also have an optimistic view of human nature. They believe people are basically honest, decent, and trustworthy.
Disagreeable individuals place self-interest above getting along with others (Smith, 2018). They are generally unconcerned with others’ well-being, and therefore are unlikely to extend themselves for other people. Sometimes their skepticism about others’ motives causes them to be suspicious, unfriendly, and uncooperative. On the other hand, agreeableness is not useful in situations that require tough or absolute objective decisions. Disagreeable people can make excellent scientists, critics, or soldiers. Its facets include trust, morality, altruism, cooperation, modesty and sympathy.
Want help to write your Essay or Assignments? Click here
Neuroticism is a trait characterized by sadness, moodiness, and emotional instability. Individuals who are high in this trait tend to experience mood swings, anxiety, irritability, and sadness (Ackerman, 2021). Those who score high on Neuroticism may experience primarily one specific negative feeling such as anxiety, anger, or depression, but are likely to experience several of these emotions.
People high in neuroticism are emotionally reactive. They respond emotionally to events that would not affect most people, and their reactions tend to be more intense than normal (Ackerman, 2021). They are more likely to interpret ordinary situations as threatening, and minor frustrations as hopelessly difficult. Their negative emotional reactions tend to persist for unusually long periods of time, which means they are often in a bad mood.
These problems in emotional regulation can diminish a neurotic’s ability to think clearly, make decisions, and cope effectively with stress (Smith, 2018).At the other end of the scale, individuals who score low in neuroticism are less easily upset and are less emotionally reactive. They tend to be calm, emotionally stable, and free from persistent negative feelings. Its facets include anxiety, anger, depression, self-Consciousness, immoderation and vulnerability (Ackerman, 2021).
Five Personality Traits
Want help to write your Essay or Assignments? Click here
Want help to write your Essay or Assignments? Click here
Big five personality theory
Personality Traits
The big five personality theory has been used in the study of personalities and research since the late 20th century. The model by Costa and McCrae has five factors: Conscientiousness, extraversion, neuroticism, openness to experience, and agreeableness.
Conscientiousness is the characteristic of being orderly and desire to perform well. Individuals who score high in the factor are; self-conscious organized, responsible, reliable, set ambitious goals and achieve them. Conversely, those who score low are less motivated, irresponsible, disorganized and less reliable (Aston, Lee & de Vries, 2014).
Want help to write your Essay or Assignments? Click here
Openness to experience is described as the ability to adapt to new methods of dealing with a life issue. According to Abel & Steve, (2018) people who score high in this factor are insightful, intelligent, curious, and imaginative and appreciate new experiences. Conversely, people who score low are closed minded, suspicious and uncomfortable to try new activities.
Big five personality theory
Extraversion is a trait that describes individuals who can interact with others and adapt to other’s viewpoints (Aston & Lee, 2014). Individuals who score high in the factor are assertive, attention seekers, energetic, talkative and socially confident. Those who score low in the aspect are usually: reserved, quiet, shy, and are intimidated being in large groups.
Want help to write your Essay or Assignments? Click here
Neuroticism is the tendency of developing proportionate worry, anxiety loneliness, and frustrations about the future. Those who score high are described to be: persistently anxious, worriers, fearful and pessimistic. Conversely, those who score low are optimistic, dynamic, and less anxious about problematic situations (Aston & Lee, 2014).
Big five personality theory
Agreeableness describes the value of being pleasant and warm to others. Those who score high are friendly, compassionate, cooperative and altruistic. Those who score low are selfish, uncooperative, suspicious and unfriendly.
The study was done on big five personality traits to assess gender differences across 55 countries. The findings indicated that women scored higher compared to men in agreeableness, neuroticism, extraversion, and conscientiousness (Terracciano, McCrae & Costa, 2014). A Similar current study done in 2015, women scored higher in extraversion and neuroticism, while men scored higher in openness to experience.
Want help to write your Essay or Assignments? Click here
Aston MC & Lee K de Vries RE (May 2014). The HEXACO Honesty-Humility, Agreeableness, and Emotionality Factors review of research and theory. Personality and Psychology Review. 18(2): 139-52
Want help to write your Essay or Assignments? Click here
Psychological Foundation of Leadership
Identify ways that a leader could use symbolic acts to strengthen a cultural value of teamwork and collaboration in the Psychological Foundation of Leadership.
and
Identify the qualities of a change leader. Also, explain how leaders can serve as role models for change. Question 1 –
Symbolic acts to strengthen a cultural value of teamwork and collaboration. Teamwork and collaboration are vital components of successful businesses and alternative ventures. Insightful leaders understand the need for developing a culture and strengthening the value of teamwork in their followers. The use of symbolism is instrumental to the strengthening of the cultural value of teamwork and collaboration.
Symbolism involves the use of actions, objects, and events to convey a targeted meaning or impart a given sense or emotion in an individual or group of people (Hambrick & Lovelace, 2017; Sergiovanni & Corbally, 1986, pp. 112 – 113; Winkler, 2009). This section identifies and expounds on several acts by leaders that serve to strengthen a cultural value of teamwork and collaboration.
Open communications Many employees consider the leadership in a corporate environment as being unreachable. Such a notion may serve to erode a sense of teamwork in the employees since they may not feel like part of a team. To address such concerns, the leadership in an office and corporate setting should find ways to foster a sense of openness in the work environment.
This could include the use of open floor plans of office space, and the abolition of the bureaucratic chain of communication between employees and management (Ford & Sturman, 2011). Such actions represent an example of a symbolic act by the organization’s leadership to show an effort toward the improvement of communication as a tool to create a culture of teamwork and collaboration.
Psychological Foundation of Leadership
Unifying tasks A critical factor in the creation of a culture that fosters teamwork and collaboration in a harmonious environment is the ability to unify different people. However, the leadership in any organization can achieve this through the creation of tasks within the workplace that create a need to collaborate with other members of the team. A case example is a development of unifying tasks that require input from various members with different skills.
In such a scenario, the leaders would not create a team but instead allow the individuals assigned to the task to seek for and collaborate with other people to complete the task. In this way, therefore, the use of unifying tasks is a symbolic gesture by leaders to strengthen the cultural value of teamwork and collaboration.
Appraising the role of each The importance and success of any leader lie with the achievement of goals by the individual followers. In this light, therefore, it is essential that the leader provide sufficient motivation for the employees. Ford and Sturman (2011) maintain that instilling beliefs, values, and norms through laws, stories, and legends are imperative to teaching culture within an organizational setting. Besides, the creation of various rituals at the workplace ensures that the followers are informed on the culture and expect the leaders to operate in a given manner (pp. 115 – 119, 123 – 124).
Such rituals may include the appraising of the best performing individuals and groups. This creates a recurring act that fosters better work morale to ensure the followers, especially when operating in a group setting strive to outperform each other. Such appraisals, therefore, not only serve to create an ongoing culture in the organization, but also help to strengthen teamwork and collaboration.
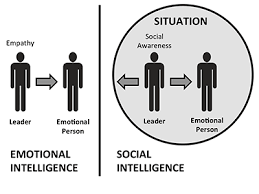
Question 2 – Qualities of a change leader Emotional intelligence To spearhead change, a leader needs to have a high level of emotional intelligence. This involves the ability to judge and control their emotions as well as discern and use the emotions of other people. In this case, active change leaders can determine the emotion and moods of their followers and act suitably. Besides, a high emotional quotient can direct the moods of their followers to allow for the right attitudes and mood for the completion of a given task. A key factor is the ability to motivate people that they can succeed at the tasks assigned to them as well as their personal lives.
Psychological Foundation of Leadership
Want help to write your Essay or Assignments? Click here
Active listening, communication, and persuasion An effective change leader is one who understands the importance of efficiency in communication. A fundamental principle of communication in such a scenario is the ability to listen to the front line people. While most leaders shut out the opinions of frontline staff, change leaders use them as critical assets to learn about the various business metrics (Dallas, 2015). Change leaders should also be able to communicate their ideas effectively to other personnel, which is vital to the implementation of the needed change. The ability to persuade people and bring them on board to accomplish the laid out ideas is essential to change leaders since not every individual is convinced of the need to change (Gleeson, 2016).
Want help to write your Essay or Assignments? Click here
Knowledge Fostering change requires adequate knowledge in the current situation, as well as the intended outcomes from the change process. Therefore, it is crucial that a change leader is knowledgeable in addition to being a seeker of information. This level of knowledgeability should not be limited to the areas of concern or operation but should be as diverse as possible. The diversity of knowledge for a change leader allows for the adoption of new skills and strategies that are applicable in their areas, which leads to growth and the achievement of the required changes. Psychological Foundation of Leadership
Accountability Change agents are responsible for not only the achievement of the required change but also for the various personnel and resources tasked under their administration. As such, a change leader requires a high level of accountability. They should be accountable for the timelines to achieve the set goals, maintaining communications and partnerships, and motivation levels among the followers among other such factors. In the same way, the change leaders demand a high level of accountability from their peers and subordinates (Rylatt, 2013)
Want help to write your Essay or Assignments? Click here
How leaders can serve as role models for change An effective change leader can serve as an example to their team as well as to other leaders. Among the ways one can serve as a role model for change is to align their words with their actions. Another is practicing self-reflection to exercise similar standards for themselves, as they demand of other people in their teams.
Establishing clear communication of requirements and goals is essential to a successful leader and is an admirable trait. Finally, the leader should show a sense of selfless empathy by being considerate of the needs and well-being of others beyond the task. With such approaches, the leader should have a presentable image that others can emulate.
Ford, R., & Sturman, M. C. (2011). Harnessing the Power of Your Culture for Outstanding Service. In J. B. M. C. Sturman (Ed.), The Cornell School of Hotel (pp. 111 – 126 ). Hoboken, NJ: Wiley Publishing.
Hambrick, D., & Lovelace, J. (2017). The Role of Executive Symbolism In Advancing New Strategic Themes in Organizations: A Social Influence Perspective. Academy of Management ReviewAcademy of Management Review, 1 – 53. Retrieved January 10, 2018, from http://amr.aom.org/content/early/2017/02/09/amr.2015.0190.full.pdf
Sergiovanni, T. J., & Corbally, J. E. (1986). Leadership and Organizational Culture: New Perspectives on Administrative Theory and Practice. Chicago: University of Illinois Press.
Want help to write your Essay or Assignments? Click here
Good parenting
Psychology Article Analysis: Good parenting heals your child’s brain
Psychology Article Analysis: Good parenting heals your child’s brain
The article ‘Good parenting heals your child’s brain,’ was written by Armin Brott and posted on hitched magazine on 21st January, 2014. It can be obtained through the following link; http://www.hitchedmag.com/article.php?id=1765
Good parenting
Main ideas
Children who grow up in institutions as opposed to with their families have cardinal brain development deficits, similar to children who grew up in poverty. Poverty brings about stress that result to damaged DNA and cells, poor immune system function, and inflammation. Orphans in institutions possess more neurological and behavioral deficits compared to those who lived in family (Brott, 2014).
At the age of for and half years, more than forty percent of the orphans had anxiety disorders while four percent had critical depressive disorders. In addition, many orphans exhibited autism signs including stereotyping and repetitive behaviors (arm-flapping and rocking).
Good parenting
Children living in institutions possess less white and gray matter (this matter connects various brain regions) compared to those in foster homes or living with their families. In addition, they have smaller amygdala and hippocampus that are vital for memory, learning, and emotion (Brott, 2014). Reduced white matter is common in a majority of the psychiatric and neurological conditions such as ADHD, schizophrenia, and autism.
A developmental neuroscientist explained that the less white matter meant less brain electrical activity- ‘alpha power’. These brain differences were accountable for the behavioral variations in the different groups of children- higher levels of anxiety and depression disorders in children in institutions (Brott, 2014). Children in foster homes and institutions had higher levels of oppositional defiant behavior and ADHD.
This gives the implication that children are placed in foster homes too late after profound deprivations had been experienced. Children can never recover from early-life isolation and the social deprivation is devastating. The environment in a child’s life between 0-5 years is vital for their future.
Want help to write your Essay or Assignments? Click here
Good parenting heals your child’s brain
Article’s purpose
The article aims at creating awareness that poverty leads to children’s stunted brain growth. However, research indicates that good parenting reverses these impacts (Brott, 2014). Therefore, there is a need for families (particularly parents) to raise their own children and avoid leaving that responsibility to the community and other people. In addition, the brain requires stimulation for development and growth.
The field of psychology explained
Autism experts, behavioralists, and developmental neuroscientists have a key role in ensuring a community with healthy people (Brott, 2014).
Analysis
Viewpoint
The article’s viewpoint is that there is a need for enriched environments during childhood and infancy. Social deprivation is the reason why children living in institutions have higher levels of anxiety and depression disorders.
Reasonable information
The article offers reasonable information owing to the fact that the information was obtained from credible researches.
Want help to write your Essay or Assignments? Click here
Is the information believable?
The information is believable since the parents were assessed keenly before the report was written. The information has also been cross examined.
Persuasiveness
The article persuades parents to practice good parenting as this plays a great role in ensuring healthy and productive children.
Information that can be added
The study should have elaborated what factors in the different environments contributed to altered brain function and structure.
Want help to write your Essay or Assignments? Click here
Elizabeth Loftus
A current and fascinating area of research is that of Elizabeth Loftus. Dr. Loftus believes that memory can be reconstructed and changed based upon outside influences and has studied misinformation effects, eyewitness testimony and memories of abuse.
Read about Dr. Loftus’ research in the textbook and go to You Tube to search for Elizabeth Loftus. www.youtube.com
There are many videos about her and explaining her research. Choose 2 videos ( Please provide links to it)which you find interesting (choose ones that have her actually speaking about her research and not copies of her experiments done by others.)
Want help to write your Essay or Assignments? Click here
Dr. Elizabeth Loftus also has her own website.
Answer the following questions in essay form (please answer and number each question separately) –
1. Explain the 2 YouTube videos that you watched about Dr. Loftus.
2. Discuss the Mini Lecture #20 article and video. Watch both parts of the video to answer the questions.
a What occurred to Jennifer Thompson and Ronald Cotton?
b How did the police investigation and procedures allow this injustice to occur?
c How have police procedures changed now?
d What are your thoughts about this story?
Elizabeth Loftus
Want help to write your Essay or Assignments? Click here
3. Discuss 3 facts that you learned about memory from reading Myers’ discussion of Memory in chapter 7 of the textbook. Cite pages of textbook.Question 1
In the first video, Elizabeth Loftus discusses the possibility of implanting a false childhood memory in a person’s mind by merely suggesting that it happened through the use of actual facts and suggestions of possibilities of what would have took place. This was done by getting background information from the subjects’ parents prior to talking to them. A quarter of this population ended up accepting the existence of the memory which was in fact false (Loftus, 2009).
In the second video, Elizabeth Loftus discusses the unreliability of eye witness testimonies. Her hypothesis or argument is that eye witness accounts are actually much more malleable than we think. This is to say that the accuracy of these events is more flexible thus making it unreliable as a source of reference for incidents that individuals have witnessed (Loftus, 2010).
Question 2
Jennifer Thompson was raped and in a bid to ensure the rapist gets justice insisted that Ronald Cotton was the one. As a result, he got convicted of a crime he did not commit and spent a decade in prison.
Police investigations allowed this injustice to occur because they relied exclusively on the eye witness account rather than other important circumstances.
Police procedures have changed in that there is more reliance on forensic evidence in combination with eye witness accounts.
This story makes me have serious doubts about eye witness testimonies and also it leads me to be sympathetic about the large number of people who have probably been convicted despite their innocence due to reliance on eye witness accounts.
Elizabeth Loftus
Question 3
The first fact I have learnt is that that there are three stages of memory formation and these are sensory, short-term and then long-term memory.
The second fact I learnt is that routine events are easy to recall because they have become automatic thus leaving very little need for effort.
The third fact I got was that sleep is indeed good for the brain (Myers, n.d.).
Want help to write your Essay or Assignments? Click here
Question 4
Memory can therefore be summarized as a the sum or recollections that an individual experiences subjectively depending on the context of the actual event as well as the present situation.