This is author biographical info, that can be used to tell more about you, your iterests, background and experience. You can change it on Admin > Users > Your Profile > Biographical Info page."
Nursing practice is bounded by various legal obligations. These laws are in accordance with the nursing ethics which guides the nature of conduct of nurses. In Australia, there is a specific nursing code of conduct that each nurse is expected to abide by in their operation. Moreover, the Parliament of Australia enacted a social act that nurses should operate within.
The primary objectives of having to adhere to legal obligations in nursing is to protect all the individuals who are affected by the nursing practice and the nurses themselves. According to Day (2007), nurses often face situations that require quick and critical decision making. In such circumstances, Carryer, et.al, (2013) argues that if a nurse fails to consider the overlaying rules regarding what to do, he or she may end up making a mistake that could be punishable by law.
For instance, the Australian rights of terminally act introduced a law which allows active voluntary euthanasia. However, this may go against the law if a nurse carries out euthanasia with consent from the family members of the sick person and not that of the sick individual. Even though the nursing legal and ethical conduct laws are different, they operate through closely related frameworks. However, nursing legal obligations regarding mental health sometimes crashers with the ethical requirement of the nursing code.
Under my specialty which is mental health, the law has set out directives of when a person can be admitted (Carryer, et.al, 2013). In the requirement, a single medical officer or nurse cannot fully ascertain that one needs to be admitted but it has to be agreed by several health officers. This legal obligations may be good in preventing unwarranted admissions, however, it sometimes contradicts with the nurses’ believe of offering help.
Mental ill individuals might not always know that they are sick, there is need for someone else to point that out. Before that happens, one cannot be treated for mental illness. This becomes problematic in a situation where there is an urgent need to treat a mental ill person yet the legal obligations procedure of ascertaining that the person is ill has not occurred.
These individuals might be involved in self destructive activities of which another person may not point out easily. Therefore, as per Doran, et.al (2015), if the proper procedure for identifying their problems is followed, treatments can be administered when it is too late. My resolution is that I will offer consultative help to the individual first before administering any medication. This way, I will be able to offer help them in advance and yet again still remain within the legal obligations confines of the Australian nursing laws.
References
Lennard-Palmer, L. (2012). The use of simulation for pediatric oncology nursing safety principles: Ensuring competent practice through the use of a mnemonic, chemotherapy road maps and case-based learning. Journal of Pediatric Nursing, 27(3), 283-286.
Carryer, J., Gardner, G., Dunn, S., & Gardner, A. (2013). The capability of nurse practitioners may be diminished by controlling protocols. Australian Health Review, 31(1), 108-15. Retrieved from http://search.proquest.com/docview/231731777?accountid=45049
Doran, Evan, BA, Grad Dip Health Soc Sci, P., Fleming, Jennifer, BA, M.H.A., PhD., Jordens, Christopher, BA, M.P.H., PhD., Stewart, Cameron L, Bec, L.L.B., PhD., Letts, J., M. Bioeth, & Kerridge, Ian H, MPhil(Cantab), F.R.A.C.P., F.R.C.P.A. (2015). Managing ethical issues in patient care and the need for clinical ethics support. Australian Health Review, 39(1), 44-50. Retrieved from http://search.proquest.com/docview/1673832440?accountid=45049
Want help to write your Essay or Assignments? Click here
In their line of duty, perioperative nurses are bound to the duty of confidentiality and ethics. However, in executing their responsibilities, perioperative nurses find themselves in dilemma situations with regards to ethical issues and confidentiality concerns accompanying the sharing of patient’s health information (Ulrich et al., 2010). According to the Nursing and Midwifery Board of Australia (2010), ensuring confidentiality of the health information of a patient I at the core of nurses establishing and maintaining trusting relationships with patients, patient’s families, and other health professionals.
With no assurance regarding the confidentiality of their health information, patients could be hesitant to provide sensitive yet important information regarding their health status/condition that can help in provision of high quality care (Price, 2015). However, perioperative nurses are faced with dilemma in situations where they consider appropriate to share a patient’s confidential health information to his or her family member(s) or caregiver for purposes of ensuring the patient continue to receive quality and safe health care.
The ethical implication of this action is the violation of ethics duty by the nurse as well as the potential loss of trust in the nurse and other health professionals in the institution by the patient or family should it be discovered that such confidential information was shared.
According to the Nursing and Midwifery Board of Australia (2010), patients have an inherent right to autonomy, which allows for their informed consent or the withheld of this consent. The law of informed consent holds that patients have the right to withhold personal information unless it is required by law to provide such information; or make decisions concerning their own treatment (Taylor, 2014).
Thus, perioperative nurses have ethical and legal obligation to respect and protect patient’s right to autonomy by allowing the patients to make their own treatment decisions or not to provide certain personal information deemed confidential. However, nurses may find themselves in a dilemma in situations where protecting and respecting patient’s right to autonomy could result in harm to the patient (Olson & Stokes, 2016).
For instance, in situations such as multiple series of surgery or uneventful incidents, letting the patient make his/ her own treatment decisions or withhold important information to health care practitioners could result in self-harm or harm others altogether.
In such scenarios, the nurse or health professional might be compelled to violate the duty of confidentiality through such means as disclosing important information concerning the patient to the family or deciding on the suitable heath care for the patient through the help of family and other health professionals without patient’s consent. This could result in an ethical break that can have legal implications on the nurse or health professional involved (Simek, 2016).
References
Nursing and Midwifery Board of Australia (2010). Nursing and national competency standards for Registered nurse. Retrieved from: http://www.nursingmidwiferyboard.gov.au
Olson, L., L., & Stokes, F. (2016). The ANA Code of Ethics for Nurses with Interpretive Statements: Resource for Nursing Regulation. Journal of Nursing Regulation, 7(2), 9-20
Price, B. (2015). Respecting patient confidentiality. Nursing Standard, 29(22), 50-57.
Simek, J. (2014). Specifics of nursing ethics. Kontakt, 18(2), 64-68
Taylor, H. (2014) Promoting a patient’s right to autonomy: implications for primary healthcare practitioners. Part 1. Primary Health Care, 24(2), 36-41
Ulrich, C., M., Taylor, C., Soeken, K., O’Donnell, P., Farrar, A., Danis, M. & Grady, C. (2010). Everyday Ethics: Ethical Issues and Stress in Nursing Practice. Journal of Advanced Nursing, 66(11). doi: 10.1111/j.1365-2648.2010.05425.x
Want help to write your Essay or Assignments? Click here
Perioperative refers to the practice of surgical procedure where patients experience surgical intervention. Perioperative nurses are tasked with the responsibility of taking care of the patient before, during and after the surgical intervention (Banschbach, 2016). During this time of surgery intervention and care, many safety issues many arise. According to Ford (2012), many safety issues such as emotional, physiological, and sociocultural safety issues may arise during the pre-operative, intra-operative, and post-operative phases of the surgical intervention because of the negligence of preoperative nurses.
Prior to the surgical procedure, perioperative nurses perform a patient assessment to evaluate the nursing care to be given in the operating room and after the patient returns to the nursing unit, or at home. This involves assessing the social, physical, and emotional needs of a patient. From the information obtained, the perioperative nurses can then predict the suitability of the surgical timing for the patient (Ford, 2012).
However, studies have shown that during this assessment period, perioperative nurses are bound to making social mistakes that result in social safety issues. According to Steelman et al. (2013) perioperative nurses, at the interaction level with the patients, may fail to actively engage the patient’s family members who can furnish important information about the patient that can help in assessing the social and physical needs of the patient and consequently help in determining the care to be provided.
In addition, Robinson (2016) states that sometimes the amount of and length of teaching recommended to a patient by the perioperative nurses is not sufficient enough to prepare the patient psychologically for the surgery type and procedure, leading to psychological safety issue during the intra-operative procedure where the patient can be more anxious and less cooperative.
According to the Nursing and Midwifery Board of Australia (2010), the information from pre-operative assessment helps in determining the surgery site and procedure for a patient. However, incorrect or insufficient information obtained from or about the patient can result in perioperative nurses recommending wrong site surgery for the patient, thereby resulting in physiological safety issue during the surgical intervention (Ford, 2012).
Besides, insufficient or inaccurate information from the pre-operative assessment can result in verification errors, scheduling errors, medication error, and patient time-out errors (from the surgical room and out of hospital) (Steelman & Graling, 2013). Thus, wrong or insufficient pre-operative assessment can be a strong basis for physical, emotional, and social safety issues on the part of the perioperative nurses.
References
Banschbach, K. S. (2016). Perioperative nurse leaders and their role in patient safety. AORN Journal, 104(2), 161-164
Ford, A. D. (2012). Advocating for perioperative nursing and patient nursing. Perioperative nursing clinics, 7(4), 425-432
Nursing and Midwifery Board of Australia (2010). Nursing and national competency standards for Registered nurse. Retrieved from: http://www.nursingmidwiferyboard.gov.au
Robinson, L. N. (2016). Promoting patient safety with perioperative hand-off communication. Journal of PeriAnesthesia Nursing, 31(3), 245-253
Pain after surgery is distressing to patients and it is an issue of concern for nurses working in PACU. Ineffective pain management during the immediate postoperative period can prolong patients stay in the PACU especially if the necessary measures are not implemented.. Nurses in PACU have a responsibility to continuously assess and give proper pain treatment to the patient (Tedore, 2015).
During my placement, I noted that nurses play an important role in management of pain during the postoperative period. Therefore they should be equipped with the proper skills and knowledge to be able to provide the best pain management. Furthermore, I realized that, despite the availability of guidelines and variety of tools for pain management, post-operative management of pain is still a challenge (Abrahamson, Fox & Doebbeling, 2012).
Moreover, increased knowledge on pharmacological and non-pharmacological pain management results in better patient outcomes. Also, these nurses should be given ample time to be able to follow the pain management guidelines to ensure proper pain management. My report aims at analyzing from the relevant peer reviewed articles on nurses’ role in management of post-operative pain and nursing issues relating to management of pain during postoperative period putting my experience in the unit into consideration.
Literature Review
Tedore, 2015 conducted a research and found out that proper management of post-operative pain benefits patients in a number of ways. Mostly it contributes to better patient comfort which is key, less cardiac complications and reduced risk of development of deep vein thrombosis and finally the patient recovers within a short period of time.
According to Wilding, Manias & McCoy, 2012 research article, it explained that that improper management of pain is majorly contributed by nurses. The factors that contribute to this include poor assessment of pain, reduced knowledge and skills on pain management, fear of side effects associated with pain management, (Wilding et al. 2012).The research conducted by (Wilding et al., 2002) explored the contributing factors to increased pain during discharge of patients from PACU.
Use of pharmacological and non-pharmacologic therapies in pain management is highlighted in an article by Joshi, Schug & Kehlet , 2014.The article outlined that morphine was mainstay for pain management in PACU. It further suggests the use of the WHO recommended ladder, starting from mild non opioids including acetaminophen and NSAIDs to strong opioids such as morphine which can be used according to severity of the pain score.
None the less, use of ice packs, distraction by use of music and positioning are some of the non-pharmacological therapies. A study was done in PACU and the findings were that use of non- pharmacological therapies together with analgesics yielded better outcomes in pain management(Joshi, Schug & Kehlet, 2014). However, the outcomes varied depending on the type of surgery performed .
According to Ramnytz, Wells & Fleming 2015, the PACU nurse has a role in assessing the associated side effects of the pharmacological agent administered. Relieving pain is the major goal of postoperative pain management and ensuring that minimal side effects results. Opioids are the mainstay of pain therapy.
However they are associated with unwanted effects such as respiratory depression, hypotension and reduced bowel movement (Ramnytz et al., 2015). In PACU, a pulse oximetry is the best tool that can be used to monitor respiratory depression during administration of opioids. However, the best method of monitoring respiratory depression is through observation of the respiratory pattern and the patient’s level of consciousness.
Methodology
During my placement in the Post Anesthetic Care Unit, I interacted and engaged the nurses in discussions pertaining their role in pain management with observations being the key technique.
Discussions
Postoperative nurses have a responsibility in assessment of pain. They should assess paints level of pain using the most effective tool to have the best outcomes. The 10 pain assessment scale is most preferred tool. However, it is important to incorporate both the subjective and objective information to be in a position to determine the most appropriate therapy for pain.
There should be continued documentation of the progress of the patient so as to determine the effectiveness of the therapy and there will be any alteration. The nurse should as well note the source and severity. In the event there is no relationship between the site and severity of pain, it will warrant investigations to determine if there is any related pathology.
Cultural background as well as anxiety is some of the patient factors determine the management of pain therefore the nurse has a responsibility of assessing them and determine if they have an effect on the patient perception. Therefore, these nurses have a role in establishing these factors.
Reflecting my placement in PACU, I appreciated that the hospital has a protocol for management of pain after surgery. For moderate pain, no opioids drugs were used while for severe pain, strong opioids were utilized. I also appreciated use of non-pharmacological therapies in pain management. Use of both pharmacological and non-pharmacological therapies increases efficiency (Ramnytz, Wells & Fleming ,2015). Non pharmacological therapies that were utilized included ice packs, music therapy and in deed they were found to be effective.
Literature suggests use of different pharmacological agent in management of pain. Similarly, during my placement, I identified those agents being utilized. For severe pain , opioids were being used while for moderate and mild pain, agents such as tramadol, diclofenac as well as acetaminophen were used.
Nurses were very vigilant and it encouraged me when they assessed the patients often after administration of these agents as the doses were given continuously until the level of pain subsided. According to WHO, recommends the use of a ladder for drug management, during my clinical placement, it was however not applied.Mariano, Miller & Salinas (2013), advocated for use of weak opioids, and NSAIDs in management of moderate pain. However, this was not practiced during my placement.
It is the nurse’s integral duty to assess the side effects of the analgesic agents. Knowledge on mode of action ,drug interaction as well as unwanted side effects so that they can be in a position to observe any side effect of the agent s and act accordingly. Likewise, I noticed that the nurses were aware of the associated side effects of the analgesic agent and they acted appropriately whenever they noticed any deviation from normal. After administration of morphine, the PACU nurses were keen to observe the respiratory pattern of patients to identify if there was any respiratory depression associated with the use of morphine.
Conclusion
My experience in management of postoperative patients in PACU enlightened me on the role of nurses in management of postoperative pain. I realized that continued provision of PACU nurses with the relevant skills and knowledge will go a long way in better management of pain after. The information I found was relevant for them included variety of pain management tools, factors influencing pain management, different therapies of pain management as well as the side effects associated with pharmacological managements. Finally I would recommend the utilization of the WHO ladder for pain management.
References
Joshi, G., Schug, S., & Kehlet, H. (2014). Procedure-specific pain management and outcome strategies. Best practice & research. Clinical Anaesthesiology, 28(2), 191-201.
Mariano, E., Miller, B., & Salinas, F. (2013). The expanding role of multimodal analgesia in acute perioperative pain management. Advances in Anesthesia, 31(1), 119-136.
Marshak, C., Bertignoli, T., Mulackal, E., Reyes, E., Duran, M., & Rojo, L. et al. (2014). Excellence in PACU pain management: How is our PACU team terforming? Journal of Perianesthesia Nursing, 29(5), e17.
McLean, G., Martin, D., Cousley, A., & Hoy, L. (2013). Advocacy in pain management: The role of the anaesthetic nurse specialist. British Journal of Anaesthetic and Recovery Nursing, 14(3-4), 43-48.
Ramnytz, L., Wells, V., & Fleming, E. (2015). An Exploration of the post-anesthesia care unit (PACU) nurses’ knowledge level of sedation scoring and pain management options. Journal of Perianesthesia Nursing, 30(4), e44.
Tedore, T., Weinberg, R., Witkin, L., Giambrone, G. P., Faggiani, S. L., & Fleischut, P. M. (2015). Acute Pain Management/Regional Anesthesia. Anesthesiology clinics, 33(4), 739-751.
Wilding, J., Manias, E., & McCoy, D. (2012). Pain assessment and management in patients after abdominal surgery from PACU to the postoperative unit. Journal of Perianesthesia Nursing, 24(4), 233-240.
Want help to write your Essay or Assignments? Click here
An individual experiencing sensory impairment may face quite a number of challenges in life. With respect to higher level needs that are defined in Maslow’s hierarchy of needs. A visually challenged individual may find it harder to actualize these higher level needs. The higher level needs that include self-actualization, self-esteem and love and belonging needs, are among the particular needs that this paper will try to elaborate on how challenging they are to a visually challenged individual to meet them.
Love and belonging is nature to most if not all human beings. These needs depict the nature of the interpersonal relationships that are adopted by most humans. However, for a Sensory Impairment person. It may be quite difficult for them to find a sense of belonging in an environment that does not favor him or her. Creating interpersonal relationships with people without actually seeing their physical appearance will be the main issue to be dealt with.
Consequently, self-esteem needs are quite important in Maslow’s hierarchy. But for a Sensory Impairment person, attaining this needs may be a challenge. They may find it extremely hard to gain confidence. It might be quite difficult for this particular individual to be able to satisfy his or her desire to be valued by other people when he or she is visually challenged.
Lastly, self-actualization needs is on the pinnacle of Maslow’s hierarchy. Self-actualization entails five key things that are key to human beings. However, for visually challenged individuals, to fully satisfy their self-actualization need may prove to be hard if the person has not yet accepted the impairment condition that faces him or her.
The nursing intervention that would be applied by a registered nurse may include the following practices. First of all when meeting the patient, the nurse will have to make a good first impression. Reason being first impression go a long way into helping visually impaired patients feel cared for.
This also helps in creating a healthy relationship between the two parties (Treas & Wilkinson, 2013). Second of all, the nurse would help the patient meet their self-esteem and self-actualization goals by helping then get to know the environment they are staying in. This would help them feel confident by not requiring aid all the time to perform the basic life activities from time to time.
Therefore, for a visually impaired individual, the attainment of the love and belonging, self-esteem and self-actualization goals may be a cumbersome task. However, with the application of the right nursing intervention by a registered nurse. The attainment of these needs in the long run may be an overcome able situation.
In recent times, it has become essential for the RN and other medical practitioners to understand the need for stroke patients in different age groups to adopt the best strategies for continuing care to them. Despite some identified similarities, there exists different needs and experiences of the young and old stroke patients. The differences are attributed to stroke effects on self-image, age normative activities, roles and the stage in the life cycle.
Some of the needs for younger patients include work disruptions, family plans, childcare responsibilities and overall disturbances of family routines (Kee et al, 2015). There is a hidden disrupted sense of self, cognitive impairment of suffering an older person’s disease among the young patients. In this case, the young patients have more unmet needs compared to their old counterparts.
The older people are at a higher risk of suffering from the stroke as compared to the young ones. Such reasons make the young patients have more specific needs both psychological and practical in nature (Kee et al, 2015). The added psychological need involves reconciling their perceived incongruity concerning suffering a disease for the old.
The old patients fail to receive constant high-intensity neurorehabilitation as compared to the young patients thus the old survivors need less therapy intensive settings (Kee et al, 2015). Compared to the old, young patients feel different about their stroke experience due to their early life stage and the effects caused by the disease.
Different psychological therapies and practices are adopted in correspondence to needs of either the old or young patients. There is a similarity between the needs of the young and old patients since both receive high amounts of therapy and specialized inpatient neurorehabilitation during their care period (Kee et al, 2015).
The therapist is an important member of the interprofessional healthcare team that would assist the RN in the provision of quality care to the stroke patient. One of the roles performed by the therapist involves promoting and teaching healthy lifestyle routines and habits to the patients to minimize the risks of secondary stroke.
Assistive technology training for the patient and home modifications requiring interventions made by the therapist are vital roles performed enhancing an effective collaboration with the RN (Kee et al, 2015). In a nutshell, adoption of the right strategies while providing care to stroke patients results to the positive and desired outcomes.
Disability is a physical or mental condition that restricts a person’s ability to move, sense or undertake activities. Disabilities can arise following an impairment of an individual’s body structure for instance loss of memory or loss of a limb in an accident. Moreover, disability can be associated with birth defects which end up affect a person in later stages of life a good example is Down’s syndrome which develops as a result of chromosome abnormalities (Huether & McCance, 2016). .
Conversely, chronic illness refers to a disease that lasts for 3 or more months and cannot be prevented by vaccines nor cured by medication. These conditions can either be acquired or inherited. An example of a chronic illness that is inherited is diabetes type I whereas hypertension is a chronic illness that may develop as a result of one having sedentary lifestyle.
They cannot be used interchangeably. This is because disability is not an illness but a body condition that impairs the body activities, and which can be as a result of sickness or a person is born with. On the other hand, chronic illness refers to a disease which attacks a person at any stage in life although a person can be born with it.
The legal implications are; the right to access of information on how to manage their disabilities and the right to resources to help them manage their disability. The legal implications are; the right to access to resources to help them manage the chronic illness as well as the right to access information on how to manage the chronic illnesses.
The actions to be implemented by RN are; providing special requirements like special education needs they should also provide comprehensive treatment plan as well as monitor the progress of individuals with chronic illness.
Chronic disease is disease that persists over a long period of time. Chronic disease can hinder independence and the health of people with disabilities, as it may create additional activity limitations. People with chronic disease often think that they are free from the disease when they have no symptoms. Having no symptoms, however, does not necessarily mean that chronic disease has disappeared.
The mining industry in Nigeria is one of great potential. It is however only just developing. Small-scale mining is an integral part of mining in Nigeria, which can contribute to local and foreign exchange earnings as well as by encouraging foreign direct investment and boosting the country’s economy. Small-scale mining is held back by a number of constraints. It is important to identify these in order develop efficient policies and strategies for its growth – which is the key to the overall development of mining in Nigeria.
This paper takes a look at small-scale mining in Nigeria, and then goes on to identify its constraints, before developing policies and strategies for its growth. A conclusion is reached and recommendations including the privatisation of the industry and a crack down on illegal mining, are made.
1. Introduction
Despite the mineral potential Nigeria possesses (proven reserves in 33 types of minerals in over 400 locations1), solid mineral exportation constitutes a mere 1% to its GDP2. This extremely low share is mainly due to Nigeria’s dependence on oil but also largely due to the underdeveloped mining sector, primarily resulting from inadequate and inefficient policies for mineral exploration development.
Over the past decade, the sector has been extensively reviewed, starting with the creation of a Federal Ministry of Solid Minerals Development in 1995. This was structured to offer a viable alternative to petroleum for foreign exchange earning as well as contributing to the country’s overall economic development. Legislation guiding all mining activities in Nigeria was also reviewed giving rise to the Minerals and Mining Decree (MMD) of 1999.
Small-scale mining (SSM) is an important part of the Nigerian mining sector, which has the potential to raise internal revenue in addition to foreign exchange, create employment and encourage foreign direct investment (FDI) via government incentives. Developing Small-scale mining is crucial to the growth of the sector, given that it is easier to break through the economic constraints as a group of small-scale miners, than for one or two small-scale miners to take on the capital and technologically intensive projects on their own. SSM is a vital stepping stone for Nigeria to fully develop this potentially vibrant sector.
However, SSM in Nigeria is severely constrained, with most current small-scale mining practices unguided and unregulated. Policies in place are inadequate, and generally small scale miners are untrained and contribute hugely to environmental degradation, and poor quality operational techniques and the loss of minerals. Most activities have gone undocumented, resulting in loss of minerals and precious stones. This has caused substantial losses in revenue to the country by way of exports, as well as through royalties and taxes.
It will be impossible to consider mining and SSM in Nigeria without putting illegal mining in perspective. Over 95% of mining activities in Nigeria are artisanal and another 95% of these are illegal3 (this includes minerals such as Tourmaline, Cabochon, Limestone, Feldspar, Tantalite, Coal, etc.4). Illegal mining is a major drawback to the sector.
It is pertinent to identify the constraints to SSM in order to determine appropriate policies and strategies for its development, which are vital to the overall growth of the Nigerian mining industry. The object of this paper is to critically assess the constraints to small scale mining in Nigeria and the steps taken so far towards its development. The paper will also consider various policies and strategies for SSM crucial to development in Nigeria. Recommendations will be made as to implementing the policies in the short and long term.
In giving comparisons of the experience of an art viewer in a real museum and an online art in a virtual museum, there is need to put considerations on the manner in which either setting is interacting with the art viewers. It is in this line that I acknowledge that there are comparative deficiencies with each setting as well as advantages. The limitations entailed in the two settings require the employment of given measures to sort the limitations and this is what is responsible for the varied presentation of art in both settings.
The physical museums are readily identifies culture. The primary function of the museums is to keep art collections that are to be accessed by the public. On the other hand, the digital art found online are in virtual museums (Pappas, 300). The virtual museums came into being following the advent of the internet as a worldwide system for communication and information delivery.
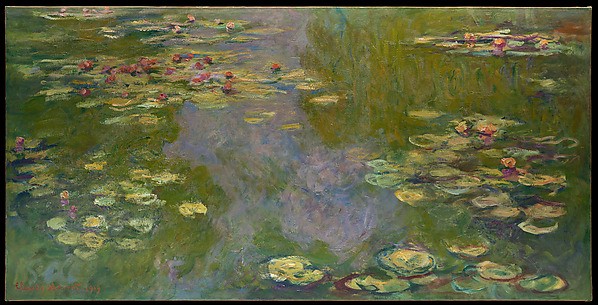
Art online; The water lilies
The pieces of art used to draw comparisons of physical viewing of art and viewing of art online are: the Water Lilies, 19919 Monet Metropolitan Museum of Art, as the physical art and the online art of Mona-Lisa. The art of Water Lilies is one among four pieces of art of water lilies that were done and completed by Monet.
The art was signed and sold in 1919. During this period, a majority of art was not yet finished and only countable paintings were made available for sale. The painting is one among a grouping of up to eleven pieces of art and they are roughly of the same size. Mona Lisa on the other hand is an oil painting done on a wood panel by an Italian painter called Leonardo da Vinci.
The main difference in viewing the painting online and visiting a museum to view one physically is that the virtual space of the art online is in two-dimension whereas being in same physical space with the art in a museum provides a three-dimensional viewing of the art. Being in the same physical space with the art enhances interaction with the piece of art. The three-dimensional aspect of physical space enhanced the line and shape of the art at the museum as it was within reach for my personal analysis even though there was no physical manipulation permitted.
The two-dimensional viewing of art online does not allow for the proper evaluation and analysis of the pieces of art as one has to use only what is provided to them on the website. The online versions of paintings have gone through editing and formatting. It is in this aspect that relying on color of the art to come up with descriptions becomes in appropriate. Texture closely borrows from this aspect of color as lighting on the art affects the texture in the view of the art viewers (DiPaola, et al. 610). I found out that I would not readily identify the painting of Mona Lisa as an oil paint mainly because I was viewing it on a screen.
Conclusively, I found out that being in the same physical space with the piece of art enhances one’s perception and they can have different angles of the art at will to come up with a personal take on the texture of the art. Viewing the piece of art online via a screen does not provide one with the ability to have the real perception of the color and texture of the art.
Works Cited
DiPaola, Steve, Caitlin Riebe, and James T Enns. “Following The Masters: Portrait Viewing And Appreciation Is Guided By Selective Detail.” Perception 42.6 (2013): 608-630. MEDLINE. Web. 29 Sept. 2016