Want help to write your Essay or Assignments? Click here
Allergic Rhinitis: Patient History
The possible disease in regard to the client’s history
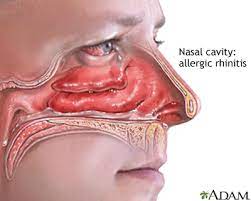
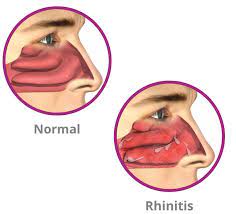
Donna’s symptoms suggest allergic rhinitis and a possible an allergic contact dermatitis. Donna complains of tenderness over maxillary sinuses and nares which are in conjunction with red, and with boggy moist mucosa and one-medium sized polyp on each side. All these symptoms suggest rhinitis, and an inflammation of the mucous membranes taking place in the nose (McCance & Heuther, 2014).
Other effects of allergens include the reddened clear and slightly swollen eyes with tearing that Donna presents with. Taking into consideration that Donna’s flaking erythematous rash is noted only on the flexor surfaces her arms, is it likely to be caused by direct contact with an allergen. A postponed sort IV extreme touchiness response Allergic contact dermatitis is and is appears localized, as opposed to widespread like atopic dermatitis (McCance & Heuther, 2014).
Questions pertaining to both personal and family history include:
Any history of pet, seasonal, or environmental allergies?
Any history of respiratory issues?
Any history of asthma or asthmatic bronchitis?
Do these symptoms present around the same time each year?
Have you noticed an irritant that causes these symptoms to flare up?
Want help to write your Essay or Assignments? Click here
Evidence suggesting that Donna doesn’t have an acute severe infection
Donna’s vital signs within normal limits, which shows hemodynamic stability; her lungs are clear to auscultation; and her postnasal drainage is clear. The presence of this evidence is not suggestive of an acute severe infection.
Type of hypersensitivity reaction involved in Donna due to her allergic Rhinitis
As described in McCance and Huether (2014, p.56), allergic rhinitis is caused by inhalants such as dust, pollen, and mold. This is classified as a Type I hypersensitivity reaction. The most common allergies are type I reactions, which happen as a response to an exposure to an environmental antigen (McCance & Huether, 2014).
Want help to write your Essay or Assignments? Click here
Breast Cancer Screening
Why is breast self-examination being replaced in the breast cancer screening guidelines by mammography and breast magnetic resonance imaging?
Breast cancer screening is normally done to facilitate early detection. This is important as it saves millions of lives in the world. According to guidelines by the American Cancer Society, breast screening should be done regularly. One of the most common and most easy methods is breast self-exam (BSE). This method has been advocated for in the recent past as it enables the women have sense of control over their breasts. Research highlights that over 70% of breast cancers incidences have been reported via BSE screening technique (Mahon, 2012).
However, there have been critiques on BSE screening method; especially due to increased incidences of benign biopsy. This is attributable to low specificity and sensitivity values. The excessive biopsies are associated with risk of cancer, emotional stress and disfiguring of the breast. The guidelines also tend to favour breast magnetic resonance imaging as well as mammography over breast self-exam method of breast screening. Magnetic resonance and mammography breast screening methods have high level of specify and sensitivity (Morrow, Waters, & Morris, 2011).
What are the risks associated with breast cancer screening? Do the risks outweigh the benefits? Why or why not?
Breast screening is important, especially for the woman in the case study as she is at high risk age. Breast screening involves process that aid in detecting breast cancer at early stage. Breast screening is done using many methods including mammogram, breast self-exam, and magnetic resonance imaging among others. Breast screening saves lives by ensuring that cancer is detected early, and appropriate interventions are made on a timely manner (Morrow, Waters, & Morris, 2011).
Want help to write your Essay or Assignments? Click here
However, there are risks involved in breast screening. To begin with, it is vital for a patient to understand that breast screenings does not prevent cancer. Some of the processes are uncomfortable and is associated with mild pain. Additionally, some processes involve use of X-rays- indicating that patients are exposed to radiation, which could lead to side effects.
However, the benefits outweigh the risks; therefore, every woman should be encouraged to undergo breast screening. There are many things that cause changes in the breast tissue. Although some of them could be harmless, it if important to get breasts checked as there is a small chance that the changes ignored are first indicator of cancer (Mahon, 2012).
References
Mahon, S. (2012). Screening for breast cancer: Evidence and recommendations. Clinical Journal of Oncology Nursing, 16 (6), 567-571. doi10.1188/12.CJON.567-571
Want help to write your Essay or Assignments? Click here
BRCA1 Gene of Breast Cancer
If you were Rachel’s healthcare provider, what would you do? Provide a rationale for your response
All the patients in the healthcare sector are privy to patient confidentiality. Physicians are not required to release any information regarding their patient to anyone without their consent. The sole purpose of having patient confidentiality is to build a good relationship between the patient and the physician. It also prevents stigmatization of patients suffering from certain disease conditions (Stephens et al., 2012).
However, there instances where patient confidentiality is breached. This occurs in cases where there is concern or safety for other individuals. This means that the disease condition affects another party which has no information regarding the disease. In the case study, Rachel is predisposed to breast cancer since it has been established that she has the BRCA1 Gene of Breast Cancer (Stephens et al., 2012). Since the gene is inherited, there is a high likelihood that both her sisters may be predisposed.
Rachel does not want her sister to know that her sister has the disease condition (Bombonati & Sgroi, 2011). As already established patient confidentiality exists between Rachel and me. However, failure to inform the other party would significantly affect their health status (Bombonati & Sgroi, 2011). Thus, in this case, I would advise Rachel to talk to both her sisters since the case will not involve patient confidentiality. If Rachel does not do so, I would advise them to talk to a different genetic counselor with the hope that she changes her mind.
BRCA1 Gene of Breast Cancer
Want help to write your Essay or Assignments? Click here
Include the pathological processes associated with breast cancer. What role does the BRCA1 gene contribute to managing the patient’s care?
Breast cancer is a multistep process that is triggered with a defect in the cell cycle that regulates how cells divide in the breast. According to Bombonati & Sgroi (2011), breast cancer is made up of four steps. The first step after the dysregulation of the cell cycle processes is the formation of a flat epithelial atypia which is progress to atypical ductal hyperplasia. After some time, it progresses to ductal carcinoma in situ before finally moving the lethal stage that is known as invasive ductal carcinoma (Bombonati & Sgroi, 2011).Once the last stage has developed the disease starts to metastasize and establishes its blood supply and other important physiologic molecules.
BRCA1 gene has been implicated in the majority of the hereditary ovarian and breast cancers. Physicians normally look for this gene mutation through the family history. Once the physicians have established that patients have these genes, the patient is genetically tested, and if the results turn out to be positive, the patient undergoes prophylactic treatment which is used to prevent ovarian and breast cancer (Bombonati & Sgroi, 2011). The presence of the gene BRCA1 assists patients to know their disease state.
Want help to write your Essay or Assignments? Click here
BRCA1 Gene of Breast Cancer
Describe and explain the role of the BRCA1 and breast cancer 2, an early onset (BRCA2) gene in contribution as a risk factor for breast cancer.
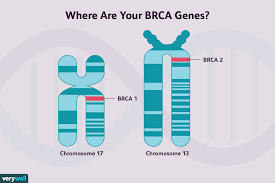
Two genes that have been identified that predispose women to breast cancer. Genetic mutations in the germline of BRCA1 gene predispose 15-45% of all cases of hereditary breast cancer. It has also been associated with 60-80% of all the breast cancer cases in women.
Additionally, it has been associated with 20-40% 0f all the ovarian cancers. Mutations associated with the gene BRCA2 have been known to have a less incidence of breast cancer. The case is low compared to that of BRAC1 (Stephens et al., 2012). Anyone associated with the gene BRAC2 has a 6% incidence of developing breast cancer in their lifetime.
Analyze the risk factors for breast cancer and possible interventions to preventive health management for women and men.
Several factors increase the risks associated with mutations in the genes BRAC1 and BRAC2. Such factors include the presence of bilateral cancer in the same women, family history of breast cancer and cases of having a genetic mutation in the BRAC1 and BRAC2 gene in the family (Stephens et al., 2012). Other factors include alcohol consumption, radiation exposure, being overweight, environmental chemicals and postmenopausal weight gain.
The first preventive measure involves undergoing breast cancer screening that can detect the presence of the gene defects associated with BRAC1 and BRAC2. Several different types of tests are available. They include mammograms, use of biopsies, clinical breast exams, hormone receptor assays and magnetic resonance imaging (Stephens et al., 2012). Early detection is key to early treatment. The other factors are easily preventable. For example, physical activity reduces incidences of being overweight.
Want help to write your Essay or Assignments? Click here
Allergy: Patient History
Donna’s symptoms suggest allergy rhinitis and a possible an allergic contact dermatitis. Donna complains of tenderness over maxillary sinuses and nares which are in conjunction with red, and with boggy moist mucosa and one-medium sized polyp on each side. All these symptoms suggest rhinitis, and an inflammation of the mucous membranes taking place in the nose (McCance & Heuther, 2014).
Other effects of allergens include the reddened clear and slightly swollen eyes with tearing that Donna presents with. Taking into consideration that Donna’s flaking erythematous rash is noted only on the flexor surfaces her arms, is it likely to be caused by direct contact with an allergen. A postponed sort IV extreme touchiness response Allergic contact dermatitis is and is appears localized, as opposed to widespread like atopic dermatitis (McCance & Heuther, 2014).
Want help to write your Essay or Assignments? Click here
Questions pertaining to both personal and family history include:
Any history of pet, seasonal, or environmental allergies?
Any history of respiratory issues?
Any history of asthma or asthmatic bronchitis?
Do these symptoms present around the same time each year?
Have you noticed an irritant that causes these symptoms to flare up?
Evidence suggesting that Donna doesn’t have an acute severe infection
Donna’s vital signs within normal limits, which shows hemodynamic stability; her lungs are clear to auscultation; and her postnasal drainage is clear. The presence of this evidence is not suggestive of an acute severe infection.
Want help to write your Essay or Assignments? Click here
Type of hypersensitivity reaction involved in Donna due to her allergic Rhinitis
As described in McCance and Huether (2014, p.56), allergic rhinitis is caused by inhalants such as dust, pollen, and mold. This is classified as a Type I hypersensitivity reaction. The most common allergies are type I reactions, which happen as a response to an exposure to an environmental antigen (McCance & Huether, 2014).
Want help to write your Essay or Assignments? Click here
Acute Tonsilitis
Subjective Data:
Name: J.W. Date: 2/27/2016 Time: Case ID #: 8008-20164545-015 Age: 35 years old Sex: Female SUBJECTIVE
CC: Patient feels sick, with multiple symptoms including skin rash, fever, headache, pain in swallowing, sore throat, abdominal pain, nausea and vomiting.
HPI:
The patient is a 35 year old female who presented to the clinic on Saturday, complaining that she has been feeling sharp pain in her abdomen and severe headache. She also notes that she has been experiencing the following symptoms sore throat, pain when swallowing food and nausea plus vomiting.
Patient is accompanied by her 15 year old daughter and 42 year old husband, who bring her to the clinic. J.W. further notes that she has fever and the symptoms began about three days ago, with the sore throat setting in suddenly. This is the first incident that the patient reports to the clinic. The patient notes that she took acetaminophen to relieve the fever and headache, but she decided to consult further treatment once she developed a skin rash.
Medications Currently in Use: Acetaminophen
Past Medical History
Allergies: Allergic to sulfa containing compounds. Had complications after using sulfonamides
Medication Intolerances: Intolerant to sulfonamides and generally sulfa containing drugs
Chronic Illnesses/Major traumas: no major illness/traumas Hospitalizations/Surgeries: No surgical history recorded; hospitalized once due to pneumonia infection Family History: No family history recorded on major illnesses; patient’s mum in good health
Want help to write your Essay or Assignments? Click here
Social History
Patient is a casual laborer living with her daughter and husband, plus her 54 year old mum. She takes her lunch from a local cafeteria, but cooks breakfast and supper at her home when she arrives from job in the evening. Her mum helps her cook food, but rarely when she is not present, ill or too tired to cook.
The patient states that she started to suspect food from the cafeteria after a change in management about a month ago. However, she continued to take lunch at the same place, but notes quality had significantly dropped. Also, she had heard a complaint from a regular customer, John, that the food was making him bloat his stomach two weeks ago though the condition disappeared without him attending to hospital.
Review of Systems General
Positive for fever: No Cardiovascular symptoms. This time she was using acetaminophen Denies chest pain, palpitations, PND, orthopnea, edema
Has a history of hx pneumonia but negative at the time of admission
Only reports for pain in her abdomen
Skin Denies bruising, delayed healing, bleeding or skin discolorations. Has no lesion changes or moles but presents with a skin rash
Respiratory Patient denies cough, breathing regular and symmetrical.
Eyes Denies eye discharge, no blurred vision, sees clearly without any aid
Gastrointestinal Reports pain in the abdomen
Ears Denies pain in ears has no ear discharge, hearing loss, or ringing in ears.
Genitourinary
Denies concerns
Nose/Mouth/Throat Positive for sore throat
Musculoskeletal Denies concerns
Breast Negative history
Neurological Denies syncope, seizures, transient paralysis, weakness, paresthesia, black out spells
Psychological: Denies depression, suicidal thoughts, irritability, sleep disturbances, and anxiety
Heme/Lymph/Endo HIV status, bruising, blood transfusion hx, night sweats, swollen glands, increase thirst, increase hunger, cold or heat intolerance Psychiatric Denies concerns
Want help to write your Essay or Assignments? Click here
Objective Data
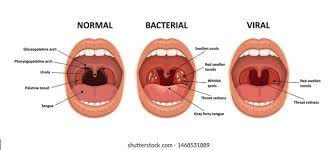
Physical exam is done in the clinic, after which the patient is sent for a lab test out of the clinic. Case is suspected to be upper respiratory bacterial infection particularly streptococcal infection. The following data is recorded from the physical exam;
General Appearance Constitutional marked as unremarkable: well developed: well nourished; no acute distress. Vital signs also noted as within acceptable limits. Patient dehydrated. General impression: A&Ox3, nicely dressed, appear appropriate, restless but cooperative, complains of chronic pain in the abdomen and headache
Skin Skin is black, warm, dry, clean and intact. No lesions noted upon examination. Scarlatiniform rashes noted HEENT Head is normocephalic, atraumatic and without lesions; hair evenly distributed.
Eyes: PERRLA. EOMs intact. No conjunctival or scleral injection.
Nose: Nasal mucosa pink; normal turbinates. No septal deviation.
Neck: Supple. Full ROM.
Pharynx redness or exudates over the tonsils noted plus erythema. Beefy red swollen uvula: Anterior cervical Adenitis and Soft Palate Petechiae noted. Teeth and gums are however unremarkable
Want help to write your Essay or Assignments? Click here
Cardiovascular S1, S2 with regular rate and rhythm. Heart location and apex is normal. No murmurs; no rubs, gallops, or click; femoral pulses normal.
Respiratory Respiratory unremarkable; respiratory rate and pattern normal; lungs clear to auscultation bilaterally.
Gastrointestinal Abdomen is soft, non tender and non-distended. No palpable masses. Liver and spleen normal; no hernias; normal bowel sounds, no bloating, only pain in the abdomen noted
Breast Chest/breast unremarkable, no masses palpitated, no redness
Genitourinary Bladder is non-distended, no UTI present
Musculoskeletal Full ROM seen in all 4 extremities as patient moved about the exam room.
Neurological Speech is clear, Good tone plus Posture erect. Balance is stable; gait normal.
Want help to write your Essay or Assignments? Click here
Assessment
Diagnostics & Lab Tests
Throat smear culture and blood specimen used
Incubation of the culture done for 48 hours before test
The suspected case is streptococcal infection by S. pyogenes or GAS
Positive rapid streptococcal test
Positive results for Antistreptolysin O test
Special Tests
Latex agglutination immunoassay test positive
Want help to write your Essay or Assignments? Click here
Assessment Findings and Plan
Diagnosis:
Patient confirmed to be having Group A Beta hemolytic Streptococcal infection, related acute pharyngitis and acute tonsilitis
Medication:
Penicillin V 500 mg tid for daily 10 days or Amoxicillin 500 mg tid for 10 days
Continue with Acetaminophen till fever completely subsidizes
Amoxicillin is a substitute in the event the patient reports to be allergic to Penicillin
Drugs to be taken orally and in full dosage given by a pharmacist
There are no generic substitutes available
Education
Advice patient to take the following measures:
Use OTC acetaminophen only for fever if relapsing occurs
Wash hands well with soap and water after using bathroom or before eating
Rinse food well and cook properly before eating
Drink water that has been purified or filtered only
Not to smoke or drink alcohol before medication is over and tests negative for GAS
If possible carry packed lunch or change the place she takes lunch from
Want help to write your Essay or Assignments? Click here
Further Notes:
The likely cause of the GAS infection is food from the cafeteria that the patient takes lunch. This, she should refrain from consuming food from the place to avoid a recurrence of the infection. High hygiene standards must be maintained to ensure zero infections to the members of her household, who include her daughter, husband and mum. Also, if convenient to her report the matter concerning the low quality food being sold at the cafeteria to public health offices, for further investigation.
Follow up Schedule
The patient is advised to report to the clinic after a week, for assessment of dosage coverage and progression of the illness. This is to ensure she completes the dosages of all medications in order to eliminate all GAS in her system and avoid development of antibiotic resistance to the Penicillin V given, which results from an incomplete dosage. In this regard, the patient should be advised strongly on the importance of completing her medications, with two follow up meetings being scheduled after a week each.
Want help to write your Essay or Assignments? Click here
Evaluation and Revisions:
The subjective and objective data was collected accordingly but the diagnostics did not cover all possible infections. Since the above are confirmatory of GAS infection, as the cause of the acute pharyngitis and acute tonsillitis, there was deemed no need to conduct tests for other upper respiratory bacteria on the cultures.
This is not only to eliminate the chances of it being a multiple infection case, but also to dictate the medicine given. This revision is necessary alongside a confirmation from the patient concerning her status in connection penicillin allergy, which should dictate the type of antibiotic given. This should be handled accordingly by the pharmacist addressing the prescription.
Metronidazole, Trimethoprim, Tetracyclines and flouroquinolones should not be used for the following reasons. Metronidazole is not effective against S. pyogenes while the patient is allergic to sulfa compounds hence Trimethoprim is contraindicated.
On the other hand, Tetracyclines pose a very high susceptibility to resistance by the bacterial species, that is GAS. Finally, Flouroquinolones are very expensive and have an unnecessary broad spectrum of activity, hence a more specific antibiotic is necessary including the above named plus Azithromycin, Clarithromycin, Clindamycin and various Cephalosporins.
Camara, M., Dieng, A., & Boye, C. S. B. (2013). Antibiotic susceptibility of streptococcus pyogenes isolated from respiratory tract infections in dakar, senegal. Microbiology insights, 6, 71.
Want help to write your Essay or Assignments? Click here
Rhinitis Patient Diagnosis
Richard presented to the healthcare facility with complaints of postnasal drainage, sneezing, rhinorrhea, and nasal congestion. These clinical manifestations are common in patient diagnosed with Rhinitis. Therefore, the Advance practitioner differential diagnoses are correct. Allergic rhinitis is most likely because patient complains of runny nose, sneezing, red itchy watery eyes, sore throat and nasal congestion (Kaliner, 2011).
This is confirmed by allergy test, nasal smear for eosinophils. It is important that the advance practitioner nurse requested for nasal smear as it helps confirm the presence of eosinophils in the nasal secretions. Presence of eosinophils indicates that the patient is diagnosed with allergic rhinitis. Blood test is also important to check for IgE antibodies which will help to confirm the diagnosis of allergic rhinitis (Dains, Baumann, & Scheibel, 2016).
Infectious Rhiniti is suspected because of patient’s signs and symptoms such as sneezing, rhinorrhoea, cough, and congestion. This is ruled out by the laboratory test findings. Non-allergic rhinitis is suspected nasal congestion, sneezing and runny nose. The immunological tests results rules out the likelihood infection (Kaliner, 2011).
Rhinitis medicamentosa is suspected due to presence of nasal congestion. This mainly occurs when the patient uses certain oral medications such as topical decongestants and some oral medications. These medications make the blood vessels to constrict causing nasal congestion. This is not likely because the patient denies use of oral medications and topical decongestants (Kaliner, 2011).
Want help to write your Essay or Assignments? Click here
Nasal speculum is also good as it helps visualize the patient’s nasal turbinate’s and mucosa. Presence of pale and boggy turbinates’ is an indicator of allergic rhiniti. However, I think further diagnostic tests should have been considered. This includes imaging tests such as CT scans to check if the patient has sinusitis, associated structural defects or chronic inflammation. Rhinoscopy should have been conducted as it would help to check for nasal polyps and associated complications (Ball et al., 2015).
Dains, J. E., Baumann, L. C., & Scheibel, P. (2016). Advanced health assessment and clinical diagnosis in primary care (5th ed.). St. Louis, MO: Elsevier Mosby.
Kaliner, M. (2011). Rhinitis. Philadelphia, Pa.: Saunders.
Want help to write your Essay or Assignments? Click here
Want help to write your Essay or Assignments? Click here
Identifying a Problem
The diagnosis and management of depression within the American population remains one of the health factors affecting the health sector. Sources determine that the prevalence of depression within the American population is ascertained to stand at 8.5%, a factor that has seen less people seek medical attention (Wagner, Müller, Helmreich, Huss, & Tadić, 2015). Thus paper therefore seeks to develop a PICOT question in determine the aspect of depression and its effects within this population.
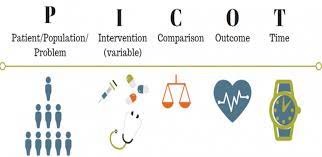
PICOT Question
It is essential to consider that the PICOT P, Population: I Intervention C, Comparison, O, Outcome and T Time is developed in guiding this study. In the American population between the ages of 30-35 of the working class (P), is there a need of developing a tool that will analyze depression (I), compared with the other approaches of care (C) that ensures appropriate procedures are developed in order to detect depression (O) within a specified time (T)? The aim of the PICOT question is developed to determine enough evidences that justify the element of depression among the American population through the use of effective tools.
Selecting Sources of Literature
In considering the results of this paper, it is essential to search through multiple databases that include EBSCOhost, Google Scholar, PsycINFO and the Cochrane and other sources from Health Care research centers. In getting the results of this study, there are key search words that need to be considered (Wagner, et.al.2015). These words include: screening, depression, depressive disorders, BECK or BDI-ii and the population. The use of both the published and the unpublished materials in searching the literatures was incorporated with the materials reviewed dating back between 2005-2010.
Selecting Sources of Literature
According to Wagner et.al.2015, a metal-analysis was conducted to determine the effects of depression on the American population. The findings of the study identifies that a majority of the population presented traumatic symptoms. This material determines that depressive disorders among the younger generation may lead to suicidal and homicidal thoughts and attempts (Jackson, Dianne & Garnefski, 2015).
Some of the symptoms that are presented by this author include chest pains, headaches, painful urination, dizziness an excessive sweating. This source intrinsically supports the specified area of study since it provides evidence to some of the effects of depression among the American population.
Want help to write your Essay or Assignments? Click here
Jackson et.al.2015 in his literature consequently revealed that the screening of depression among the American population undergoes a process of identification, assessment, and initiation of approaches aimed at managing this disease within the American population (pp.197). This author details a quantitative randomized study within this population and establishes that the abuse of substances is as a result of depression, a factor that explains the reasons why several Americans engage in risky sexual behaviors.
On the other hand, the population is also likely to engage in drugs and substance abuse as a result of depression. The author determines that there is a need of developing a concurrent treatment method that uses psychotropic drugs and other stable stimulants in the management of depression. The inclusion of psychotherapeutic method is also essential in the management of depression.
The author also mentions that depression within this population needs to be effectively managed since discoveries have been made that establish individuals in this state engage in unprotected sex and the inclusion of multiple sexual partners, a factor that would result into a health concern within a nation.
References
Wagner, S., Müller, C., Helmreich, I., Huss, M., & Tadić, A. (2015). A meta-analysis of cognitive functions in children, adults and adolescents with major depressive disorder. European Child & Adolescent Psychiatry, 24(1), 5-19. doi:10.1007/s00787-014-0559
Want help to write your Essay or Assignments? Click here
Diabetes Mellitus
Being newly diagnosed with diabetes mellitus can be overwhelming and confusing due to the several things that a patient needs to learn and understand. However, for millions of diabetic patients learning about their diabetes is the first step towards living a longer and healthier life. According to Shaw (2014), Registered Nurses (RNs) play an important role of educating individuals that have just been diagnosed with diabetes mellitus encouraging them that they can live longer if they follow important guidelines for managing diabetes.
First, the RN should let the patient understand what type 1 diabetes is and how its symptoms present by highlighting the classic symptoms associated with diabetes mellitus such as excessive thirst and hunger, fatigue, unexplained weight loss, nausea, and vomiting. She should encourage the patient that he is not the only one suffering from type I diabetes.
Most youth with type 1 diabetes do not adhere to clinical guidelines (Wood et al, 2013). Therefore, the nurse can use examples of patients of almost similar age to the patient and are coping well with diabetes mellitus. The nurses should also explain to the patient that insulin injections are the central treatment for type I diabetes and for the patient to lead a quality life she should adhere to her medication.
For proper management of type I diabetes, some of the factors that the RN should focus on mainly includes control of blood glucose, insulin management, nutrition, exercise, and support (Atkinson, Eisenbarth & Michels, 2014). The nurse should advise the patient to measure his blood glucose levels regularly and administer insulin appropriately. Exercise on the other hand is a significant component of proper care for type I diabetes as it aids the body to respond with more stable levels of blood glucose (Haas et al., 2013).
Want help to write your Essay or Assignments? Click here
However, patients should be cautioned against extreme exercise which lowers their glucose levels considerably. Additionally, the nurse should aid the patient understand how various foods affect blood glucose and enlighten them on how to come up with solid meal plans (Chiang et al., 2014). She should also encourage the patient to seek help from other people with the same condition and be free to visit the medical center in case of any clarification.
The steps of the teaching learning process that were most likely not well employed are the implementation and the evaluation steps. In the implementation step, the nurse should have delivered content in a manner that is more organized with the aid of planned teaching strategies. The evaluation step could be improved if the nurse questioned the patient on some aspects such as why insulin is important in management of type I diabetes and more so the rationale of giving it as an injection instead of pills.
References
Atkinson, M. A., Eisenbarth, G. S., & Michels, A. W. (2014). Type 1 diabetes. The Lancet, 383(9911), 69-82.
Chiang, J. L., Kirkman, M. S., Laffel, L. M., & Peters, A. L. (2014). Type 1 diabetes through the life span: A position statement of the American Diabetes Association. Diabetes Care, 37(7), 2034-2054.
Haas, L., Maryniuk, M., Beck, J., Cox, C. E., Duker, P., Edwards, L., … & McLaughlin, S. (2013). National standards for diabetes self-management education and support. Diabetes care, 36(Supplement 1), S100-S108.
Shaw, R. J., McDuffie, J. R., Hendrix, C. C., Edie, A., Lindsey-Davis, L., Nagi, A., … & Williams, J. W. (2014). Effects of nurse-managed protocols in the outpatient management of adults with chronic conditions: a systematic review and meta-analysis. Annals of internal medicine, 161(2), 113-121.
Wood, J. R., Miller, K. M., Maahs, D. M., Beck, R. W., DiMeglio, L. A., Libman, I. M., … & T1D Exchange Clinic Network. (2013). Most youth with type 1 diabetes in the T1D Exchange Clinic Registry do not meet American Diabetes Association or International Society for Pediatric and Adolescent Diabetes clinical guidelines. Diabetes care, 36(7), 2035-2037.
Want help to write your Essay or Assignments? Click here
Want help to write your Essay or Assignments? Click here
Introduction
There is an increased focus on geriatric dermatology due to the growing trend towards aging populations in several countries across the globe. Elderly individuals are predisposed to many dermatological conditions as a result of senile changes in their skin. Although sometimes skin problems seem to be minor compared to major chronic diseases frequently seen in elderly patients, proper diagnosis and management aids in reducing the morbidity and influences positively their quality of life.
How to Properly Diagnose Skin Wounds in Frail Elders
Diagnosis is based on patient history. It is also founded on physical examination whereby a physician inspects the appearance of the condition, mode of distribution, arrangement and configuration, size of individual lesion, color. Surface characteristics such as rough, smooth, waxy or warty, and shape which can either be oval, round, or linear. Diagnostic tests can also be carried our such as skin scrapings that are important in detecting fungal infections, skin prick tests for allergies, and skin biopsies.
In an infection, germs are present in the body and are responsible for signs and symptoms such as pus from wounds, fever, and increased leukocyte count. Conversely, in colonization germs are present in the body but the patients do not present any signs and symptoms.
Type of Skin Wound
I selected herpes. This is an infection caused by the herpes simplex virus. Individuals with this infection have sores anywhere on their skin. Usually, it occurs around the nose, mouth, genitals, and buttocks. The infection is a painful experience, embarrassing and recurs time after time. Herpes is generally associated with genital herpes. However, herpes is actually a term referring to a family of viruses ranging from Epstein-Barr virus (causes infectious mononucleosis), varicella zoster virus (causes shingles), herpes virus 1/HSV-1, to herpes virus 2 HVS-2. Under a microscope, HSV-1 and HSV-2 look identical. Either type can infect the genitals and the mouth.
Herpes simplex has been ranked as one of the most common infections with approximately one out every five individuals in US having HSV-2 and about half to three quarter of all adults having a positive test for HSV-1. However, just ten percent of exposed persons get visible sores.
During the infection, the viruses, HSV-1 and HSV-2, traverse into the nerves where they blend with the DNA forcing the body to make copies of them so that they can be spread easily to other people. However, the body’s immune system attacks the viruses and the products overcoming them. In individuals with a weakened immune system, the virus traverses to the skin where it leaks out in tiny blisters that are painful, burning or unusually tender.
Herpes infection is severe in individuals whose immune system is weak such as children and the elderly. Often, it is a mild infection in that it goes unnoticed in majority of the people who are infected. The infected persons perceive the infections as normal skin irritation or chaffing. However, HSV can recur years later and be mistaken as an initial attack resulting in unfair accusations of infidelity between partners.
Want help to write your Essay or Assignments? Click here
Treatment
Anti-viral pills such as acyclovir, famyclovir, and valacyclovir are used in treatment herpes. Topical application ointments also help in reducing the healing time as well as the duration of symptoms. Some of the topical applications that are prescribed include penciclovir, acyclovir, and docosanol cream.
There are several risk factors in geriatric dermatology that can predispose one to developing herpes. Some of these factors include, a history of a prior sexually transmitted infection, engaging in sexual intercourse at an early age, having several sexual partners, and poor socioeconomic status. Research by Bernstein et al., (2013) indicated that HSV-2 is transmitted easily from men to women than vice versa. This explains why females have a high likelihood of developing HSV-2 infection than men. Individuals whose immunity is compromised such as patients with HIV are also at a high risk of acquiring herpes infection.
Prevention
Herpes is a contagious infection whose prevention before and after an outbreak is of great significance. If signs of recurrence such as itching, tingling, burning or tenderness are felt at any area of the body, then that area should be kept away from other people. Patients that have mouth lesions should avoid sharing cups, lip makeup, or kissing. Sharing of towels and clothing should be avoided strictly.
Avoidance of sexual activity among patients with genital herpes is an important intervention. Sharing of sexual toys should also be avoided highly as they may promote transmission of herpes. Use of condoms is the most effective intervention of preventing herpes transmission. Partners should also go for medical check-ups in case one of them experiences herpes symptoms.
Conclusion
Individuals who have had the infection should maintain general good health and keep stress as low as possible to lit chances of having recurrences which fortunately are milder than the initial attack. Infected patients should take care of the affected skin area by keeping it dry and clean during outbreaks to facilitate healing. Physical contact should be avoided until all skin sores heal completely, not just scabbed-over.
If one touches a sore he/she should wash hands thoroughly with soap and water failure to which the hands can transmit the virus to other body parts such as eyes causing herpes keratitis a condition that causes pain and sensitivity to light and is accompanied with discharge. Geriatric dermatology practice has to be by professional who have studied and understand their geriatric patients.