Want help to write your Essay or Assignments? Click here
Locate the Best Evidence
Clinical Practice Guidelines used in the practice setting
Among the bodies in the US that are tasked with the responsibility of developing the clinical practice guidelines include the AADE (American Association of Diabetes Educators) that published the Standards of Practice, Scope of Practice, as well as the Standards of Professional Performance of Diabetes Educators. Based on these documents and evidence, pharmacists have a particular role of delivering diabetes education.
AADE also came up with a framework related to optimal practice for self management. During the process, there should be an assessment of the specific education needs in every patient (Garber, Gross & Slonim, 2010). Second is the identification of the particular diabetes self-management goals in every person. This can go a long way in ensuring effectiveness of the strategies used.
Third, the behavioral interaction as well as the education should aim at ensuring that the individual achieves the identified self-management goals (Kapoor & Kleinbart, 2012). In addition, following the education sessions, there should be evaluations aimed at determining the extent to which the individual is achieving the identified self-management goals.
The other body accountable for creating the clinical practice guidelines is ADA (American Diabetes Association). According to this body, the care standards or recommendations should not preclude clinical judgment but should be applied within an excellent clinical care context, with adjustments being made for comorbidities, individual preferences, as well as patient factors. The body also emphasizes on patient education that is patient-specific (Kapoor & Kleinbart, 2012).
Want help to write your Essay or Assignments? Click here
Information for conducting systematic reviews
One aspect that can guide the systematic review is evidence supporting self-management training’s effectiveness for diabetes type 2, especially on a short-term basis. Second is evidence showing that education programs that are based on the health belief model are effective in improving self-management (Chijioke, Adamu & Makusidi, 2010). Therefore, their implementation can promote effectiveness in preventing the disease’s complications.
Proper diabetes health education has short-term impacts such as knowledge of diabetes and glycemic control. Health policy makers should consider the need to train diabetes educators so that they can tailor fitting education interventions among the patients (Garber, Gross & Slonim, 2010).
Want help to write your Essay or Assignments? Click here
Published research sources- journals to be used
The use of peer-reviewed articles will be cardinal in helping locate credible information. Majorly, those articles are evidence-based and can ensure quality information. The journals will be obtained from authentic databases such as Proquest, GoogleScholar, and Elsevier. Research sources can also be obtained from nursing bodies’ sites as these also deliver quality information.
Experts in the US who provide sources of best evidence
Entities or bodies such as the ADA and AADE are among the experts who promote best evidence. Moreover, individuals, particularly those in the healthcare sector have a cardinal role in spreading best evidence. Moreover, agencies, particularly those focusing on research, help in generation and promoting the use of best evidence.
My personal expertise and how it fits with the EBP
Diabetes type 2 patients need to develop a wide array of competencies so that they can manage being in greater control of their disease. in connection to this, while education should promote health, it should respect the voluntary choices and self-perceived needs.
Although there is the possibility of educating patients towards greater autonomy, a good number of professionals are not ready to collaborate with them. moreover, clinical staff should acquire better comprehension on diabetes management and of the theoretical principles that underlie patient empowerment. These factors need to be considered for effective EBP (Mshunqane, Stewart & Rothberg, 2012).
Kapoor, B., & Kleinbart, M. (2012). Building an Integrated Patient Information System for a Healthcare Network. Journal of Cases on Information Technology (jcit), 14, 2, 27-41.
Garber, J. S., Gross, M., & Slonim, A. D. (2010). Avoiding common nursing errors. Philadelphia: Wolters Kluwer Health/Lippincott Williams & Wilkins.
Chijioke, A., Adamu, A. N., & Makusidi, A. M. (2010). Mortality patterns among type 2 diabetes mellitus patients in Ilorin, Nigeria : original research. Journal of Endocrinology, Metabolism and Diabetes in South Africa, 15, 2, 79-82.
Want help to write your Essay or Assignments? Click here
Want help to write your Essay or Assignments? Click here
Nurse Managers Career Planning
Nurse Managers have demanding and complex responsibilities that involve coordinating work of individuals with varying education, skills, and personalities of providing safe, high quality patient care. The Nurse managers are accountable for staff performance, resource utilization, financial management, and patient outcomes. The Nurse Managers also ensure that patient care is delivered in line with the standards of practice and organizational ethics and policies. According to Anonson et al., (2014), good nurse managers provide leadership and ensures that his/her department runs smoothly.
After evaluating myself with the skills inventory, I found that I have the various strengths and weakness in the following areas;
Personal and Professional Accountability
First, I noted that I am competent enough when it comes to personal growth and development. This is because I hold a Bachelors OF Science Nursing (BSN) degree which has equipped me to meet the demands weighed on today’s nurse. With this degree, I have acquired skills in critical thinking, case management, and health promotion in order to practice across various inpatient and outpatient settings. I also possess leadership skills that are crucial for anyone that would like to serve as a nurse manager. In my practice, I adhere to the expected nursing codes of ethics.
However, I am a novice when am required to make appropriate decisions surrounding the several ethical dilemmas in my practice. For instance, a teen who had been diagnosed with syphilis due to unprotected sex asked me to lie to her mum about her condition. Moreover, I am also an active member of several nursing associations such as the American Nursing Association (ANA); an important institution that safeguards our welfare as nurses.
Want help to write your Essay or Assignments? Click here
Career Planning
I am an expert in this area because I understand my role as a BSN nurse and what is expected of me. I also intend to pursue a master’s degree in Nursing. However, I have not yet decided on the program I need to pursue.
Personal Journey Disciplines
I noted that I am an expert in this area. I have vital management skills that can aid me in educating and supervising staff without micromanaging. I can use conflict resolution and negotiation skills to enhance collaboration between physician, staff, and clinical leaders. I can also mentor and coach stuff at all levels. Moreover, I am flexible hence I can adapt quickly in the field of healthcare as patients usually develop problems. However, I find it a bit challenging to make agent decisions of care on my own in accordance to the changing needs. I prefer consulting someone else before I can implement a decision.
Reflective practice reference behaviors/tenets
After rating myself on this area, I found that I uphold integrity and transparency in all my dealings. I also have the desire of developing my potential. For instance, I usually challenge myself to attain the standards that some of my predecessors in the field of nursing have set. This aids me to discover my potential, know my weaknesses and strengths whenever I want to attain certain goals.
However, I do not know how to create and maintain a balance that renews and regenerates my spirit and body so that I can grow continually. This is because I usually find myself being caught up in the profession, squeezing some personal time relax and rejuvenate has always been a challenge to me risking work burn out.
Reflective practice is one of the most important pillars in my career. It aids my making sense of human frailties such as mental and physical health and the dynamics between the relationship between human beings and the system in which they function.
Want help to write your Essay or Assignments? Click here
Often, leaders are charged with the responsibility of creating change processes in an organization (Schaffer et al., 2013). Change processes that involve upgrade of tools and techniques, human resources, and basic rules and controls within a hospital are the mandate of managers within the organization. With my leadership set, I will be able to make the change initiatives real and tangible rather than abstract.
I will also ensure that I awaken the enthusiasm and ownership of the proposed change within the organization. My leadership set also helps me to be accountable for filling the gap between strategic decisions and the certainty of executing the change within the workforce and structure of the institution. I will use my communication skills to ensure that the staff is updated on all change activities that are taking place and what we expect to achieve.
Thinking strategically is one of the goals for my leadership growth. I intend to improve my ability of seeing the big picture and learn to step back from daily tactical details of my practice and concentrate not only on the “how” and “what” but also on the “why.”By being a critical thinker, I will hold all my views and reasoning to intellectual reasoning standards. This will aid in reducing ambiguity and confusion in the understanding of ideas and thoughts. Achievement of this goal will place me at a suitable position thinking deeply and broadly. My thinking will be driven towards being adequate, precise, and logical for my intended purpose.
Schaffer, M. A., Sandau, K. E., & Diedrick, L. (2013). Evidence‐based practice models for organizational change: overview and practical applications. Journal of advanced nursing, 69(5), 1197-1209.
Want help to write your Essay or Assignments? Click here
Want help to write your Essay or Assignments? Click here
Chronic care model
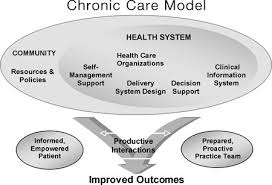
The chronic care model refers to an organizational approach through which people suffering from chronic diseases can receive care in the primary care settings. It is population-based. Moreover, it creates supportive, evidence-based, and practical interactions between the activated, informed patient and proactive, and prepared practice team.
This model identifies some vital healthcare system elements which promote care for chronic diseases that is high-quality. Within the elements, there are particular change concepts, which are used by the team to guide the improvement efforts. The care redesign processes applied agree to the change concepts.
In the same way, the aim of the patient-centered medical home is ensuring that the patients receive better care (Varkey, 2010). The model focuses more on patient needs. Some of the aspects through which care access can be improved include increased communication between the patients and providers through telephone and email, and extending the office hours. The elements of the chronic care model increase care coordination as each contributes in its own way.
One of the goals of the patient-centered medical home is also increasing care coordination. Moreover, the latter model aims to enhance the overall quality and reduce costs simultaneously (The Commonwealth Fund, 2009).
The patient-centered medical home model has a keen focus on the whole person, and different healthcare professionals participate in the care provision. There aspects are not focused on the chronic care model where attention is solely on the chronic disease. Similar to the chronic care model, the patient-centered medical home model integrated all health care aspects for overall health improvement. A unique characteristic of the patient-centered medical homes is that patients seek care from personal physicians who lead care teams within the medical practice (National Business Coalition on Health & National Health Leadership Council, 2010).
Want help to write your Essay or Assignments? Click here
Elements that are most significant for achieving safety and quality goals
The patient-centered medical home model
This model also has some elements that promote achievement of its set goals. These are physician-led practice, whole-person orientation, coordinated and integrated care, access, and focus on safety and quality. These elements have to interact for the care being provided to be relevant. Same as the chronic care model, evidence-based medicine is given a lot of emphasis as it helps improve the patient outcomes. Moreover, the care team has to offer comprehensive care that is both coordinated and integrated (Institute for Healthcare Improvement, n.d.).
Chronic care model
This model identifies the cardinal elements that every healthcare system should have for high-quality care for chronic diseases to be realized. The elements are as follows; clinical information systems, decision support, delivery system design, self-management support, health system, and community. Under each element, there are evidence-based change concepts and in combination, they foster interactions that are productive and meaningful between informed patients that are very active in their health and well-being and providers with expertise and resources.
Based on this model, these elements should all interact for chronic diseases to be managed and prevented effectively. In essence, the factors in the community that contribute to chronic diseases should be addressed and measures taken to promote safer communities (Varkey, 2010). In addition, patients should engage in self-care and management; healthcare delivery should be safe, personalized, and high-quality; the best decisions should be made for better care provision; and the clinical side should also be effective.
As such, chronic diseases can be prevented and managed appropriately. All the elements of this model are important for safety and quality goals. Each of them has a cardinal contribution, and ignoring any would result to inefficiencies.
Want help to write your Essay or Assignments? Click here
Structuring the models to achieve the best medical outcomes for individual patients at the lowest cost to society
In relation to the chronic care model, the organizations being created should be committed to offering high quality and safe care. Basically, the business plan of the health system should reflect a dedication to applying the model across the organization. Moreover, the clinical leaders should ever be dedicated and visible members whose roles performance should be perfect. Again, the community resources should be mobilized so that the patients’ needs can be met. As a result, the chronically ill patients can be kept active, involved, and supported.
Moreover, it is necessary that the patients are prepared and empowered to as to participate in their healthcare. The delivery system design should assure self-management support and effective, efficient care. Birenbaum (2011) indicated that the decision support should promote care that agrees to patient preferences and scientific data. In relation to the clinical information systems, data should be organized to promote effective and efficient care (Varkey, 2010).
For the patient-centered medical home model to be effective, the team of providers have to cooperate. In addition, there has to be payment reform and health information technology. Considering that medical homes might be virtual or physical network of services and providers, there has to be health information technology that can facilitate information sharing and communication among providers. In addition, the providers receive financial incentives that enables them focus on quality as opposed to volume.
References
Birenbaum, A. (2011). Remaking chronic care in the age of health care reform: Changes for lower cost, higher quality treatment. Santa Barbara, Calif: Praeger.
National Business Coalition on Health, & National Health Leadership Council. (2010). Patient-centered medical home: Has the time come? : National Health Leadership Council, Portland, ME, June 22-24, 2010. Washington, D.C: National Business Coalition on Health.
Want help to write your Essay or Assignments? Click here
Mental Health Consumer Care
“How would you feel when almost every individual within the society treats you differently by avoiding any form of interaction? Well, no one prefers to be treated that way. Mental health consumers are more often marginalized because of their mental state. This aspect can worsen their entire being and situation, which can propel them to neglect the self. By definition, a mental health consumer refers to persons who use mental health services in order to empower their mental health status while obtaining support or treatment.
Evidently, suffering from mental illness can be devastating to a patient and that situation can affect various aspects of their lives ranging from their physical status to their emotional being. On the other hand, self-neglect refers to the behavioral situation in which a person neglects or fails to attend to their personal basic needs such as feeding, appropriate clothing, tending appropriately to medical conditions, feeding or personal hygiene. Nonetheless, in extreme cases of self-neglect, the situation can be inferred to as Diogenes syndrome (Townsend, 2013).
Despite the severity of self-neglect in a mental health consumer, nursing professionals need to care for them in an attempt to improve their mental health issues. This presentation focuses on the relevance of nursing care of mental healthcare consumers who self-neglect to modern mental health nursing as well as to recognize the appropriate linkages with other mental health care providers.
In order to appropriately identify patients suffering from mental health problems, it is ideal to identify the various aspects that help in identifying them or the factors that assist in characterizing them. Most cases involving self-neglect are often recognized as a result of numerous complaints received from several sources such as community organizations, neighbors, GPs and healthcare professionals (Naik, Lai, Kunik & Dyer, 2008).
The process of managing and identifying cases is very complex and difficult, which requires a multi-disciplinary and multi-agency approach. Based on several studies, individuals with mental health problems are often poor and indulge in smoking habits, lack exercise, consume alcohol, have poor diets and consumer other drugs (Middleton, 2008; Richardson, 2007). The deteriorating state of their daily lives often affects their energy levels, organization skills, attention, physical abilities or motivation.
The effect on the patient can cause them to neglect the self. Studies also indicate that the side effects of certain psychiatric medications can cause a decrease in the motivation levels among mental patients (Townsend, 2008; Gunstone, 2003). Therefore, self-neglect among mental patients can be caused by illness alone. With the help of medical practitioners including nursing care cases of self neglect among mentally ill patients re likely to reduce.
Want help to write your Essay or Assignments? Click here
Notably, nurses constitute the largest population of health care professionals, thus, they have a key role in the management and identification of self-neglect among mentally ill patients. The relevance of nursing care to mental healthcare consumers in the modern nursing practice can be identified through the assessment, diagnosis, outcome identification, planning, and implementation and evaluation steps (Peate, Wild, & Nair, 2014).
In the initial process, nurses establish a database in which the database relates to the client using assessment tools such as KELS, geriatric depression scale and nutrition assessment (Pickens et al., 2007). The next process involves identifying the patients’ health care needs as well as the specific goals for care. The third process involves establishment of the specific criteria that measures the achievement of anticipated outcomes while the forth process involves designing the most appropriate strategy that facilitates the achievement of the desired goals.
The implementation process involves initiating and finishing actions that are necessary in accomplishing goals as the final process involves determination of the degree to which the objectives and goals of the implemented care have been achieved (Boyd, 2010). Through this sequential step, a nursing practitioner is capable of analyzing personal achievements in relation to providing care to patients, especially those with mental illness and having self-neglect. The outcomes of this process help both the nursing specialists and other medical professionals to identify the various steps that in deed help in solving the problem of self-neglect among mentally ill patients, for future referencing.
Currently, the nursing profession is working towards providing holistic care to patient. This means that other than assisting patients within hospitals, nurses also help patients outside the hospitals such as acceptance within the society. With reference to mentally ill patients, they are among the mostly segregated groups of people within the society. The nursing education helps in providing additional knowledge to nurses and it is disseminated to the public by informing them that mentally ill patients are just like other people with slight differences in their ways of thinking and making decisions.
Some of the interventions include adult protection services, drug misuse rehabilitation, housing services, budgeting services and neurological assessment among many others (Lauder, Anderson & Barclay, 2005). These shape the current approach in providing care to patients by integrating friendly approaches towards the patients. By dealing with cases of self neglect, nurses are capable of reducing the stigma that mental patients receive, which in turn promotes their general well-being.
In conclusion, within the modern nursing field, practitioners are more propelled towards the identification and management of self-neglect cases among mentally ill patients as a means of preventing the reoccurrence of the phenomenon. Since nurses constitute the largest portion of individuals within the health care sector, they play a chief role in ensuring the provision of proper care to patients.
In the nursing profession, taking care of mentally ill patients helps in identifying the most appropriate ways of providing care. Treating mentally ill patients with self-neglect issues helps in improving the health of the patients in general.”
Lauder, W., Anderson, I., & Barclay, A. (2005). A framework for good practice in interagency interventions with cases of self-neglect. Journal of Psychiatric and Mental Health Nursing, 12, 2, 192-198. http://www.ncbi.nlm.nih.gov/pubmed/15788037
Pickens, S., Naik, A. D., Burnett, J., Kelly, P. A., Gleason, M., & Dyer, C. B. (2007). The utility of the Kohlman evaluation of living skills test is associated with substantiated cases of elder self-neglect. Journal of the American Academy of Nurse Practitioners, 19, 3, 137-142. http://www.ncbi.nlm.nih.gov/pubmed/17341281
Want help to write your Essay or Assignments? Click here
New Graduate Nurse (NGN)
Transitioning from a student into a professional practitioner is a difficult experience for most people. However, the transition experience is especially difficult for graduate nurses who are ushered into a demanding work environment. Most new nurses are shocked at the sheer contrast between student life and work. Just a few weeks after employment, Graduate nurses are expected to take up serious responsibilities including patient care and supervisory duties.
This review explores literature on the New Graduate Nurse (NG) transition experience with the aim of discovering shortcomings in this knowledge area. This research hopes to bridge the gap in knowledge about self-care strategies that NGNs can use as the transition to Registered Nurses.
Background
Waves of research have studied the experiences of nurses as they transit from student to practicing Registered nurses. The first research wave focused on the experiences of individual nurses during the transition phase. The second wave, investigated the effectiveness of interventions meant to support nurses during the transition. Most studies into the experience of New Graduate Nurses (NGNs) used survey and interviews to arrive at their conclusions. The studies reported that NGNs initially found the role of practicing nurse extremely stressing and they reported many challenges.
However, role stress decreased as NGNs gained confidence, obtained clinical support and developed competence (Casey, Fink, Krugman, &Propst 2004; Halfer& Graf, 2006). NGNs described the transition as a difficult time filled with feeling or incompetence, fear of physicians, an overwhelming sense of responsibility, and difficulties in prioritizing, organizing or delegating tasks. Bowles and Candela (2005) carried a study in Nevada that sought to find the attrition rates of new nurse.
It was reported that approximately 30% of NGNs quit their first nursing jobs within the first year of employment. In just two years, 57% had moved from their first jobs. According to Bowles and Candela (2005), the high nurse turnover hinders work productivity, quality patient outcomes and the morale of the staff. Moreover, high turnover means healthcare organization have to incur the cost of rehiring and retraining new nurses to take the roles of those who leave.
While training more nurses may solve the nurse shortage problem, the problem of deficient patient care and supportive work environment needs to be handled to smooth the nurse transition. Casey et al (2004) found that NGNs are not satisfied with their working environment as they lamented the lack of a consistent preceptor, struggles with authority, a feeling of being undervalued, and workload issues. Chi, Laschinger and Wong (2006) carried out a study on transition among 226 nurses with less than 2 years practice experience.
The study reported similar results to Casey et al (2005); they indicated that there were high burnout rates among new nurses. The nurse complained about the lack of support, limitation of access to resources and opportunities as their main barrier to productivity at the transition phase. However, the job satisfaction outcomes of NGNs improved significantly after the first 18 months of practice. Halfer and Graf (2006) reported high job satisfaction rates among 84 subject of their research.
The two authors argued that nurse started to enjoy their work once they were able to organize their time, prioritize tasks, access resource, understand job expectation, and were made aware of the availability of professional development opportunities. Studies of nursing thought processes also indicate support the conclusion that the transition is a stressing time for graduate nurses.
According to Pellico, Brewer and Kovner (2009), NGNs’ confidence was initially low as they were unsure about the experience and knowledge , they also feared the interaction with patients as they felt they would not be able to understand their issues. NGNs were also worried about acting autonomously and deciding when it was necessary to call physicians. By the 9 month, NGNs had significantly boosted their confidence and were able to make competent patient care decisions.
The research wave on NGNs’ transition experience was followed by studies that investigated institutional initiatives to smooth the transition. The second wave was concerned with the preceptor and recognized him/her as a crucial component of the NGN transition process (Bowles and Candela, 2005). This phase of research proposed formal classes; evidence based practice, and guidance and mentoring as crucial precepts of nursing practice.
The studies proposed that all medical care should be involved in precepting, the presence of a designated preceptor and rewards for those who successfully carry out the preceptor’s role (Bowles and Candela, 2005). Some studies indicated that extended residencies and structured orientation to support the NGN transition improved job satisfaction and reduced the high nurse turnover. NGNs have complained about limited orientation, disorientation, feelings of confusion and loss, overwhelming responsibility as the main barriers to successful transitions.
The difficulties of the NGNs transition to practice are further complicated by other changes in their life (Scott, Engelke and Swanson, 2008). NGNs may have moved to a new town, become married or changed schools. Obviously, the new nurse transition face is fraught with difficult and there is need for support and self-management strategies to handle the stresses of this phase of a nurse’s career.
Want help to write your Essay or Assignments? Click here
Experiences of New Nurses
NGNs transitioning issues can be classified into four broad themes; demands on nurses, support at the workplace, the control of their role as employees, and perceptions of self efficacy (Bowles and Candela, 2005).
Workplace Demands
Demand in the workplace on new nurses is a theme that has been explored by many studies. NGNs identified workplace demands such as staff shortages, workload, decision making responsibilities and administrative duties as overwhelming issues (Casey et al, 2004). A survey of newly licensed nurses around the US found that demands relating to time were among the most stressing issues for NGNs. Nurses complained that they were often required to work hard or fast by their supervisors.
Casey et al (2004) also noted that nurses found it stressing to take responsibility for patient care provided by unregulated staff. Unfortunately, nursing has the dubious distinction of being the only profession which requires new practitioners to assume supervisory duties. Studies exploring the expectations of the multidisciplinary team working with new nurses reveal too high expectations of the (NGNs Waite, 2004). At eight weeks, the multidisciplinary team studied in the research expected new nurses to be able to make specific clinical assessments, be able to use laboratory data, and be able to react to emergencies (Dyess and Sherman, 2009).
In addition, the team expected the NGNs to be knowledgeable about the whole health systems. Many employers have complained about the deficit of key skills and the readiness of NGNs to deal with the demanding clinical environment. NGNs critical thinking skills and approaches to medication administration have also been called into question by some scholars. Romyn et al (2009) argued that NGNs are often responsible for near misses and medication errors as they are not proficient enough handle the medication demands of the job.
According to Edwards et al (2015), the concerns about the competence of NGNs are not unwarranted as competent performance is not guaranteed while working with graduate nurses. The lack of a consistent system to measure the performance of NGNs also further complicates the expectation of competence placed upon them. One of the common criteria for measuring competence in nursing is speed and ability to complete specific tasks (Romyn et al, 2009).
Unfortunately, the speed of New Graduate nurses may be quite low and they may not have the same capability to handle patient issues as experienced nurses (Delaney, 2003). This method of evaluating the performance of NGNs sees their work condemned as unsatisfactory and is often associated with stress among the new graduates joining the workforce.
Want help to write your Essay or Assignments? Click here
Control
Many NGNs report concerns about the control or autonomy of their new roles as practicing nurses. Many new nurses complained that being responsible and accountable to patients was stressing (Delaney, 2003). Duchscher and Cowin (2004) pointed out student nurse roles did little to equip NGNs for the responsibilities awaiting them in practice. Duchscher and Cowin (2004) support the view that patient care decision and outcome responsibilities often overwhelm new nurses.
However, the reactions of the NGNs varied as some embraced the new responsibilities, but most reported a feeling of being overwhelmed (Delaney, 2003). Researchers have argued that control is a double edged sword in the transition period. For nurses who embrace responsibility and accountability easily, it is exhilarating and exciting. In contrast, control brings about a feeling of anxiety for nurses who are unprepared for the new responsibilities.
NGNs may also suffer disorientation and poor sense of control as a result of unfamiliarity with the practice environment. NGNs are surprised when they realize that the practice environment is significantly different from the school context (Duchscher, 2001). Chang and Hancock (2003) argue that NGNs can experience as a result of uncertain expectation of the new role which gives rise to role ambiguity.
Support
Support by supervisors or coworkers plays a significant role in easing the NGN transition process. Often NGNs expend much effort in trying to familiarize themselves with existing workers in their healthcare setting (Casey et al, 2004). Duchscher and Cowin (2004) note that NGNs are in need the support of other members of the multidisciplinary team. Majority of NGNs report that there are adequately supported by preceptors and colleagues (Delaney, 2003).
They also reported that they felt part of the team. However, new nurse could not challenge established ways of doing things as they lacked support in doing this. Nurses also need support from family and friends outside the workplace. In fact, nurse reported that they performed better when they received support from outside the workplace.
Want help to write your Essay or Assignments? Click here
Self-efficacy
Casey et al (2004) reported that NGNs feel incompetent and inadequate as they begin practicing as nurses. Many new nurses report feeling as if they did not posses the necessary skills or knowledge to work as Registered Nurses (Delaney, 2003; Duchscher and Cowin, 2004). NGNs also greatly doubted their clinical competence as they lacked a frame of reference unlike experienced healthcare workers (Duchscher and Cowin, 2004). Duchscher and Cowin (2004) points out those NGNs felt their inadequate knowledge was a serious limitation. However, NGNs reported higher self-efficacy and confidence scores as they continued to gain clinical experience.
Want help to write your Essay or Assignments? Click here
Transition Impacts
Job stress
Job stress is one of the most widely reported results of the NGN transition (Delaney, 2003; Duchscher and Cowin, 2004; Twibell et al 2012; Pellico, Brewer and Kovner, 2009). Despite the emphasis on job stress in many studies, few have investigated the intensity of stress affecting NGNs. Chang and Hancock (2003) reported that the transition experience resulted in moderate amounts of stress among NGNs. According to Casey et al (2004), NGNs comfort and confidence is initially very high as the new graduates join the profession, however, it decreases with time in the job.
Fortunately, nurse comfort and confidence starts to increase as they gain experience and peaks one year after commencing practice. Chang and Hancock (2003) reported that nurses experience many stressors during the transition process. According to the two, the initial stressors include role ambiguity and responsibilities. After one year of employment, the main stressor is role overload.
Job Satisfaction
One of the most ignored outcomes of NGN transition is the job satisfaction impact. Common studies have emphasized on the challenges experienced during the transition phase but rarely have the satisfying job aspects being explored. Delaney (2003) reported that some new nurses reported that they found their new roles as practicing nurses satisfying. Nurse’s satisfaction with their work increased when they started to recognize available opportunities for personal growth and development.
Some NGNs reported that it felt exciting to finally take up the role of a practicing nurse. However, NGNs also reported many dissatisfying elements in their work, these included dizzying pace of work, inadequate staffing and too much autonomy and responsibility (Pellico, Brewer and Kovner, 2009; Casey et al, 2004; Chang and Hancock, 2003). Nurse who were satisfied with their work also were also more intent on staying with their employer.
Further research explored job satisfaction as an independent variable and presented interesting research findings. Delaney (2003) reported that nurses who were satisfied with their jobs felt a strong sense of belonging to the organization. Satisfaction in jobs was also negatively associated with role stress, role ambiguity and conflict during the transition process (Chang & Hancock, 2003).
Research has also explored outcomes such as turnover intent and nurse turnover. Many of these outcomes increase when there is shortage of nursing manpower. A high patient:nurse turnover is likely to precede and increase in patient mortality and has been indicated as an accelerator of nurse burnout (Bowles and Candela, 2005). Nurses report that the main causes of high turnover among NGNs are poor work design and emotional exhaustion.
These result support the need to research into self-management strategies that nurses can use to cope to the stressing experiences of the transition process. Twibell et al (2012) have hypothesized that self-care strategies may help nurse achieve higher levels of satisfaction with their jobs.
Interventions to support NGNs
Decades of research have popularized the notion that NGN transition is a process that needs to be addressed (Bowles and Candela, 2005). Many interventions have been applied to assist is making the transitioning process easy. However, there are few reports of intervention that aim to teach nurses how to self-manage the transition by performing recommended self-care practices.
Early studies recommended the use of internship programs and preceptor pairing to expose the nurse to the “real world” prior to commencing practice (Bowles and Candela, 2005). However, the value of preceptor and internship programs have come into questions recently and new research is needed to clarify the value they add to the NGN transition process.
One of the gaps in NGN transition research is the lack of measurement of the effectiveness of interventions to support NGN transition (Bowles and Candela, 2005). Many of the early studies, presented subjective results of the effectiveness of the interventions they were studying. Later studies in the late 1980s started to include quantitative measures of the effectiveness of the interventions (Casey et al 2004). However, most of the studies failed to measure the impact of the studies on patient outcome. Some of these studies are included in this review.
Want help to write your Essay or Assignments? Click here
Conclusion
The NGN transition process is a well researched area within the nursing profession. Most stakeholders seem to be aware of the problems that face NGNs as they transition into their practice. Decades of research present findings detailing mostly ineffective interventions to deal with the NGN transition process. One of the most common intervention experimented in research was the use of internship, residencies and preceptors. However, many researchers call into question the usefulness of these interventions in addressing the problems of new nurse’s commencing practice.
This research reveals two reasons why intervention to smooth the NGN transition failed to work despite decades of research. First, the early interventions were never objectively evaluated and thus the opportunity to gauge their effectiveness and increase their impact was missed. Furthermore, most of the intervention were designed to address problems identified in specific health care settings and were not backed by an understanding of the issues facing NGNs.
Few of the interventions sought to get to the bottom of the stress experienced by NGNs. Secondly, the interventions failed to take into consideration the many elements of the practice environment. This review presents some of the environmental factors that lead to a difficult experience for NGNs transitioning to practice. NGNs perception of their own abilities and knowledge is among the most stressing factors.
Many NGNs feel incompetent and inadequate when there are starting out. This attitude contrast sharply to the work demand, high expectation, and responsibility that characterize their work environment. Other healthcare workers expect nurses to exhibit the same level of competence and skills as experienced practitioners less than two months after being employed.
Few nurses are prepared for the sudden responsibility and autonomy they have over patient care decision. Many find the new responsibility overwhelming and are stressed. However, a substantial number of new nurses are excited and exhilarated to work autonomously. This review also indicates that support from colleagues, supervisors, family and friends are important for a successful transition. Nurses who receive support express confidence in their ability, Skills and knowledge.
This review has revealed that the NGN transition process can be an extremely stressing period. Many studies point to the stress and emotional distraught that is experienced by NGNs during the transition. Most studies report that new nurse feel overwhelmed by the demands of the new environment, feelings of inadequacy and fear of failure. Very few studies have investigated the possible positive impact of self-care mechanism that may assist nurse’s cope with the difficult transition period. This research will seek to address this gap in research and provide valuable evidence that may be used to improve the NGN transition experience significantly.
References
Bowles, C., & Candela, L. (2005). The first job experiences of recent RN graduates. Journal of Nursing Administration, 32(3), 130Y136.
Casey, K., Fink, R. R., Krugman, A. M., & Propst, F. J. (2004). The graduate nurse experience. Journal of Nursing Administration, 34(6), 303-311.
Cho, J., Laschinger, H., & Wong, C. (2006). Workplace empowerment, work engagement and organizational commitment of the new graduate nurses. Nursing Leadership, 19(3), 43Y60.
Duchscher, J. E. B., & Cowin, L. S. (2004). The experience of marginalization in new nursing graduates. Nursing Outlook, 52(6), 289-296.
Dyess, S. M., & Sherman, R. O. (2009). The first year of practice: New graduate nurses’ transition and learning needs. The Journal of Continuing Education in Nursing, 40(9), 403-410.
Edwards, D., Hawker, C., Carrier, J., & Rees, C. (2015). A systematic review of the effectiveness of strategies and interventions to improve the transition from student to newly qualified nurse.International journal of nursing studies, 52(7), 1254-1268.
Halfer, D., & Graf, E. (2006). Graduate nurse perceptions of the work experience. Nursing Economics, 24(3), 150.
Pellico, L. H., Brewer, C. S., & Kovner, C. T. (2009). What newly licensed registered nurses have to say about their first experiences.Nursing outlook, 57(4), 194-203.
Romyn, D. M., Linton, N., Giblin, C., Hendrickson, B., Houger Limacher, L., Murray, C., … & Weidner, A. (2009). Successful transition of the new graduate nurse. International Journal of Nursing Education Scholarship, 6(1).
Scott, E. S., Engelke, M. K., & Swanson, M. (2008). New graduate nurse transitioning: necessary or nice?. Applied Nursing Research,21(2), 75-83.
Twibell, R., St Pierre, J., Johnson, D., Barton, D., Davis, C., Kidd, M., & Rook, G. (2012). Tripping over the welcome mat: Why new nurses don’t stay and what the evidence says we can do about it. American Nurse Today, 7(6), 357-365.
Waite, R. (2004). Psychiatric nurses: Transitioning from student to advance beginner RN. Journal of the American Psychiatric Nurses Association, 10(4), 173-180.
Want help to write your Essay or Assignments? Click here
Want help to write your Essay or Assignments? Click here
Hospice Nurse Transition
Business Plan
Executive Summary
Transitioning from a student into a professional practitioner is a difficult experience for most people. However, the transition experience is especially difficult for graduate nurses who are ushered into a demanding work environment. Most new nurses are shocked at the sheer contrast between student life and work. Just a few weeks after employment, Graduate nurses are expected to take up serious responsibilities including patient care and supervisory duties. This business plan sets out to bridge the gap in knowledge about self-care strategies that NGNs can use as they transition to hospice.
Business Plan-Transitioning Nurses into Hospice
1.0 Preliminary
1.1 Objectives
The business plan aims to educate the nurses that are transitioning into hospice on how to identify, explore, and improve our health and self-care practices. The plan will also help teams to evaluate risks for burnout and compassion fatigue, and learn more effective strategies for work and home-life balance. The self-management transition plan hopes to decrease attrition rates to zero in the next six months.
1.2 Philosophy Background
Hospice can be defined as a model of care formulated to afford comfy, and support to the patient as well as families especially when a life-limiting malady does not react to remedial prescriptions. The philosophywas startedin 1960 by Dr. Cicely Saunders, a British physician. The phrase “hospice” comes from the Latin word “hospital” that implies guesthouse. Today there are more than 4,100 hospice programs that offer this specialized care to patients.
1.3 Problem Statement
While the demands for hospice service are greater than the resources, it leads to nurses being put into the field to care for these patients too soon. However, experience demonstrates that nurses who transition into hospice are thoroughly orientated and trained on how to care for dying patients. In short, nurses tend to care deeply for others, at their peril. The underlying cause is that the nursing orientation and training lacks on self-care and time management, which ultimately results in compassion fatigue and high attrition for nurses in hospice. There is, however, there is a need to equip hospice transitioning NGNs’ with “Self-Management skills to decrease compassion fatigue and attrition rates.
2.0 Situation on the Ground
The Georgetown Hospice office is growing at a rapid rate in their patient census and so is the attrition rate with the nurses. This situation forces the current nurses to take on larger caseloads and more on call. Nurses are being hired, but most are new to the field of hospice, which requires some extra training. Often this training and orientation are not completed, due to the need of the new nurse in the field to help with patient coverage (Casey et al.2004).
The incomplete orientation can cause nurses to feel unsupported, inadequate and insecure. These feelings and emotions without the necessary skills or training on self-management lead to burnout, compassion fatigue and high attrition. Developing this self-management project will, in turn, help this office and company as a whole by saving the cost of new hires.
3.0 Critical Assumptions and Constraints
The Georgetown Hospice Leadership Team has all agreed that this self-management project will be essential to manage the growth of the office (Dyess & Sherman, 2009). The Leadership Team believes this project will build up the moral and confidence in the nurses. Decrease the amount of physical, psychological and emotional exhaustion felt by the nurses (Scott, Engelke & Swanson, 2008).
Predict the risk of compassion fatigue and give the tools to be successful in the field. This project will require collaboration and feedback between the Executive Director, Quality Manager, Manager of Clinical Practice and the RN Case managers. Some constraints are:
Conflicts in the nurses schedules- not all be able to meet at the same time
Inadequate nursing coverage- high patient to nurse ratio
Poor communication- limited feedback
Want help to write your Essay or Assignments? Click here
4.0 Key Success Factors
Educate the staff on coping strategies for facing death with assigned patients.
Encourage effective communication between managers and staff.
Schedule RN Case-mangers with sensible ratios that will allow the nurse to spend adequate time with patients to build rapport.
Incorporate burn-out prevention strategies in every monthly nursing meeting.
Team building to show the nurses a sense of belonging.
Teach Nurses to safeguard their boundaries.
Want help to write your Essay or Assignments? Click here
5.0 NGNs’ Experiences
Nurses experience difficulties when transitioning from student to practicing Registered Nurses. NGNs initially find the role of practicing nurse extremely stressing and challenging. However, role stress decrease as NGNs gain confidence, obtain clinical support and develop competence (Duchscher & Cowin, 2004).NGNs describe the transition as a difficult time filled with feeling or incompetence, fear of physicians, an overwhelming sense of responsibility, and difficulties in prioritizing, organizing or delegating tasks.
Approximately 30% of NGNs quit their first nursing jobs within the first year of employment. In just two years, 57% had moved from their first jobs (Duchscher & Cowin, 2004). The high nurse turnover hinders work productivity, quality patient outcomes and the morale of the staff. Moreover, high turnover means healthcare organization have to incur the cost of rehiring and retraining new nurses to take the roles of those who leave.
While training more nurses may solve the nurse shortage problem, the problem of deficient patient care and supportive work environment needs to be handled to smooth the nurse transition. However, NGNs are not satisfied with their working environment as they complain about the lack of a consistent preceptor, struggles with authority, a feeling of being undervalued, and workload issues (Delaney, 2003). There are high burnout rates among new nurses.
The nurse also complains about the lack of support, limited access to resources and opportunities as their main barrier to productivity at the transition phase. However, the job satisfaction outcomes of NGNs improve significantly after the first 18 months of practice. Nurses start to enjoy their work once they can organize their time, prioritize tasks, access resource, understand job expectation, and were made aware of the availability of professional development opportunities.
The transition is a stressing time for graduate nurses. NGNs’ confidence is initially low as they are unsure about the experience and knowledge; they also fear the interaction with patients as they feel they will not be able to understand their issues. NGNs are also worried about acting autonomously and deciding when it is necessary to call physicians (Twibell et al. 2012). Therefore, this business plan will demonstrate how to boost NGNs confidence and ability to make informed decisions about service delivery.
6.0 Management Summary
Key stakeholders for the project has been identified and interviewed to obtained and assess their requirements/needs, as well as input for successful implementation. Key stakeholders include Executive Director; Jackie Williams, Quality Manager; Anna Hamilton, Manager of Clinical Practice; Aneko Jackson and Manager of Clinical Practice Tracy Sudduth. All requirements were obtained, reviewed, prioritized, and approved by the project sponsor and team members(Bowles & Candela, 2005). Key Stakeholders, Executive Director; Jackie Williams, Quality Manager; Anna Hamilton, and Manager of Clinical Practice Tracy Sudduth, will be updated on a weekly basis in person or via telephone regarding the progress of the business plan.
Want help to write your Essay or Assignments? Click here
7.0 Strategy and Implementation
7.1 Strategies
7.1.2 Control
Many NGNs are concerned about the control or autonomy of their new roles as practicing nurses. In addition, they complain that being responsible and accountable to patients was stressing. Student nurse roles are inadequate in equipping NGNs for the responsibilities awaiting them in practice. Patient care decision and outcome responsibilities often overwhelm new nurses (Romyn et al.2009).
However, the reactions of the NGNs vary as some embrace the new responsibilities, but most report a feeling of being overwhelmed. Control is a double-edged sword in the transition period. For nurses who embrace responsibility and accountability easily, it is exhilarating and exciting. In contrast, control brings about a feeling of anxiety for nurses who are unprepared for the new responsibilities.
NGNs may also suffer disorientation and poor sense of control as a result of unfamiliarity with the practice environment. NGNs are surprised when they realize that the practice environment is significantly different from the school context (Chang & Hancock, 2003). NGNs can experience as a result of the uncertain expectation of the new role which gives rise to role ambiguity.
7.1.3 Support
Support by supervisors or coworkers plays a significant role in easing the NGN transition process. Often NGNs expend much effort in trying to familiarize themselves with existing workers in their healthcare setting. Moreover, NGNs are in need the support of other members of the multidisciplinary team. The majority of NGNs report that there are adequately supported by preceptors and colleagues, which makes them part of the team (Cho, Laschinger & Wong, 2006).
However, the new nurse cannot challenge established ways of doing things as they lack the necessary support. Nurses also need support from family and friends outside the workplace. In fact, nurse reports that they perform better when they receive external support.
Some of the interventions to support NGNs include teaching nurses to self-manage the transition by performing recommended self-care practices. The use of internship programs and preceptor pairing to expose the nurse to the “real world” before commencing practice is also effective (Halfer & Graf, 2006). Nonetheless, NGN transition research lacks anadequate measure of interventions to support the process.
7.1.4 Self-efficacy
NGNs feel incompetent and inadequate as they begin practicing as nurses. Many new nurses report feeling as if they do not possess the necessary skills or knowledge to work as RNs. NGNs also greatly double their clinical competence as they lack the basis, unlike experienced healthcare workers. Furthermore, NGNs feel that their inadequate knowledge was a severe limitation (Edwards et al, 2015). However, NGNs have a higher self-efficacy and confidence scores as they continue to gain clinical experience.
7.2 Implementation
There are three options considered in the development of this Self- Management Project.
1. Weekend training carried out once a month that would only focus on the well-being of the RN Case Managers (other disciplinary team members would also be welcomed). This time, would allow the nurses to reflect on challenges and solutions as a team (Pellico, Brewer & Kovner, 2009).
2. Develop a month long structured orientation that includes a week of orientation that is dedicated to healthy coping mechanisms in the field of hospice.
3. Incorporate the self- management education in the monthly nursing meetings and encourage a brief self-evaluation on current feelings and emotions weekly during IDG meetings.
After discussing all three options with the sponsors, option 3 was the most feasible and would not change the budget since these meetings are already included in the budget during the nurses normal work hours. Option one sounds good, but it defeats the purpose which is self-management; we want our nurses happy, we want them to relax when they are off and enjoy with their families.
This also increases the budget for extra overtime (Waite, 2004). A month-longorientation forces our veteran nurses to work that much longer with the high patient to nurse ratios. High ratios are very stressful to these nurses. We want our nurses to enjoy their employment with the company and allow them the opportunity to give quality care to patients.
Want help to write your Essay or Assignments? Click here
8.0 Financial Plan
8.1 Budget Estimate and Financial Analysis
The cost of this project is no added cost to the budget since the sponsors have requested that execution of this project is incorporatedinto the standard meetings.
8.2 Schedule Estimate
The Georgetown office has determined this is a critical need, due to the rapid growth in the census; therefore, the projection is to be completed by May 1, 2016. A time estimate has been provided to the project sponsors, and will be the responsibility of the Project Champion, to ensure the expected completion date is obtained.
9.0 Conclusion
The nursing career has a plethora of challenges especially for NGNs, who complain of limited orientation, disorientation, feelings of confusion and loss, overwhelming responsibility as the primary barriers to successful transitions. The difficulties of the NGNs transition to practice are further complicated by other changes in their life. The truth is that the new nurse transition face is fraught with difficult, and there is a need for support and self-management strategies to handle the stresses of this phase of a nurse’s career.
This care plan hinted about training to help fix anomaly. Formal classes; evidence-based practice, and guidance and mentoring as crucial precepts of nursing practice. As such, all medical care should be involved in presenting, the presence of a designated preceptor and rewards for those who successfully carry out the preceptor’s role. Again, extended residencies and structured orientation to support the NGN transition may improve job satisfaction and reduce the high nurse turnover.
Want help to write your Essay or Assignments? Click here
Casey, K., Fink, R. R., Krugman, A. M., & Propst, F. J. (2004). The graduate nurse experience. Journal of Nursing Administration, 34(6), 303-311.
Chang, E., & Hancock, K. (2003). Role stress and role ambiguity in new nursing graduates in Australia. Nursing & health sciences, 5(2), 155-163.
Cho, J., Laschinger, H., & Wong, C. (2006). Workplace empowerment, work engagement and organizational commitment of the new graduate nurses. Nursing Leadership, 19(3), 43Y60.
Delaney, C. (2003). Walking a fine line: Graduate nurses’ transition experiences during orientation. Journal of Nursing Education, 42(10), 437-443.
Duchscher, J. E. B., & Cowin, L. S. (2004). The experience of marginalization in new nursing graduates. Nursing Outlook, 52(6), 289-296.
Dyess, S. M., & Sherman, R. O. (2009). The first year of practice: New graduate nurses’ transition and learning needs. The Journal of Continuing Education in Nursing, 40(9), 403-410.
Edwards, D., Hawker, C., Carrier, J., & Rees, C. (2015). A systematic review of the effectiveness of strategies and interventions to improve the transition from student to newly qualified nurse.International journal of nursing studies, 52(7), 1254-1268.
Halfer, D., & Graf, E. (2006). Graduate nurse perceptions of the work experience. Nursing Economics, 24(3), 150.
Pellico, L. H., Brewer, C. S., & Kovner, C. T. (2009). What newly licensed registered nurses have to say about their first experiences.Nursing outlook, 57(4), 194-203.
Romyn, D. M., Linton, N., Giblin, C., Hendrickson, B., Houger Limacher, L., Murray, C. & Weidner, A. (2009). Successful transition of the new graduate nurse. International Journal of Nursing Education Scholarship, 6(1).
Twibell, R., St Pierre, J., Johnson, D., Barton, D., Davis, C., Kidd, M., & Rook, G. (2012). Tripping over the welcome mat: Why new nurses don’t stay and what the evidence says we can do about it. American Nurse Today, 7(6), 357-365.
Waite, R. (2004). Psychiatric nurses: Transitioning from student to advance beginner RN. Journal of the American Psychiatric Nurses Association, 10(4), 173-180.
Want help to write your Essay or Assignments? Click here
Want help to write your Essay or Assignments? Click here
Transition Experience of New Graduate Nurses
Transitioning from a student into a professional practitioner is a difficult experience for most people. However, the transition experience is especially difficult for graduate nurses who are ushered into a demanding work environment. Most new nurses are shocked at the sheer contrast between student life and work. Just a few weeks after employment, Graduate nurses are expected to take up serious responsibilities including patient care and supervisory duties.
This review explores literature on the New Graduate Nurse (NG) transition experience with the aim of discovering shortcomings in this knowledge area. This research hopes to bridge the gap in knowledge about self-care strategies that NGNs can use as the transition to Registered Nurses.
Background
Waves of research have studied the experiences of nurses as they transit from student to practicing Registered nurses. The first research wave focused on the experiences of individual nurses during the transition phase. The second wave, investigated the effectiveness of interventions meant to support nurses during the transition. Most studies into the experience of New Graduate Nurses (NGNs) used survey and interviews to arrive at their conclusions. The studies reported that NGNs initially found the role of practicing nurse extremely stressing and they reported many challenges.
However, role stress decreased as NGNs gained confidence, obtained clinical support and developed competence (Casey, Fink, Krugman, &Propst 2004; Halfer& Graf, 2006). NGNs described the transition as a difficult time filled with feeling or incompetence, fear of physicians, an overwhelming sense of responsibility, and difficulties in prioritizing, organizing or delegating tasks. Bowles and Candela (2005) carried a study in Nevada that sought to find the attrition rates of new nurse.
It was reported that approximately 30% of NGNs quit their first nursing jobs within the first year of employment. In just two years, 57% had moved from their first jobs. According to Bowles and Candela (2005), the high nurse turnover hinders work productivity, quality patient outcomes and the morale of the staff. Moreover, high turnover means healthcare organization have to incur the cost of rehiring and retraining new nurses to take the roles of those who leave.
While training more nurses may solve the nurse shortage problem, the problem of deficient patient care and supportive work environment needs to be handled to smooth the nurse transition. Casey et al (2004) found that NGNs are not satisfied with their working environment as they lamented the lack of a consistent preceptor, struggles with authority, a feeling of being undervalued, and workload issues. Chi, Laschinger and Wong (2006) carried out a study on transition among 226 nurses with less than 2 years practice experience.
The study reported similar results to Casey et al (2005); they indicated that there were high burnout rates among new nurses. The nurse complained about the lack of support, limitation of access to resources and opportunities as their main barrier to productivity at the transition phase. However, the job satisfaction outcomes of NGNs improved significantly after the first 18 months of practice. Halfer and Graf (2006) reported high job satisfaction rates among 84 subject of their research.
The two authors argued that nurse started to enjoy their work once they were able to organize their time, prioritize tasks, access resource, understand job expectation, and were made aware of the availability of professional development opportunities. Studies of nursing thought processes also indicate support the conclusion that the transition is a stressing time for graduate nurses.
According to Pellico, Brewer and Kovner (2009), NGNs’ confidence was initially low as they were unsure about the experience and knowledge , they also feared the interaction with patients as they felt they would not be able to understand their issues. NGNs were also worried about acting autonomously and deciding when it was necessary to call physicians. By the 9 month, NGNs had significantly boosted their confidence and were able to make competent patient care decisions.
The research wave on NGNs’ transition experience was followed by studies that investigated institutional initiatives to smooth the transition. The second wave was concerned with the preceptor and recognized him/her as a crucial component of the NGN transition process (Bowles and Candela, 2005). This phase of research proposed formal classes; evidence based practice, and guidance and mentoring as crucial precepts of nursing practice.
The studies proposed that all medical care should be involved in precepting, the presence of a designated preceptor and rewards for those who successfully carry out the preceptor’s role (Bowles and Candela, 2005). Some studies indicated that extended residencies and structured orientation to support the NGN transition improved job satisfaction and reduced the high nurse turnover. NGNs have complained about limited orientation, disorientation, feelings of confusion and loss, overwhelming responsibility as the main barriers to successful transitions.
The difficulties of the NGNs transition to practice are further complicated by other changes in their life (Scott, Engelke and Swanson, 2008). NGNs may have moved to a new town, become married or changed schools. Obviously, the new nurse transition face is fraught with difficult and there is need for support and self-management strategies to handle the stresses of this phase of a nurse’s career.
Experiences of New Nurses
NGNs transitioning issues can be classified into four broad themes; demands on nurses, support at the workplace, the control of their role as employees, and perceptions of self efficacy (Bowles and Candela, 2005).
Workplace Demands
Demand in the workplace on new nurses is a theme that has been explored by many studies. NGNs identified workplace demands such as staff shortages, workload, decision making responsibilities and administrative duties as overwhelming issues (Casey et al, 2004). A survey of newly licensed nurses around the US found that demands relating to time were among the most stressing issues for NGNs. Nurses complained that they were often required to work hard or fast by their supervisors.
Casey et al (2004) also noted that nurses found it stressing to take responsibility for patient care provided by unregulated staff. Unfortunately, nursing has the dubious distinction of being the only profession which requires new practitioners to assume supervisory duties. Studies exploring the expectations of the multidisciplinary team working with new nurses reveal too high expectations of the (NGNs Waite, 2004). At eight weeks, the multidisciplinary team studied in the research expected new nurses to be able to make specific clinical assessments, be able to use laboratory data, and be able to react to emergencies (Dyess and Sherman, 2009).
In addition, the team expected the NGNs to be knowledgeable about the whole health systems. Many employers have complained about the deficit of key skills and the readiness of NGNs to deal with the demanding clinical environment. NGNs critical thinking skills and approaches to medication administration have also been called into question by some scholars. Romyn et al (2009) argued that NGNs are often responsible for near misses and medication errors as they are not proficient enough handle the medication demands of the job.
According to Edwards et al (2015), the concerns about the competence of NGNs are not unwarranted as competent performance is not guaranteed while working with graduate nurses. The lack of a consistent system to measure the performance of NGNs also further complicates the expectation of competence placed upon them. One of the common criteria for measuring competence in nursing is speed and ability to complete specific tasks (Romyn et al, 2009).
Unfortunately, the speed of New Graduate nurses may be quite low and they may not have the same capability to handle patient issues as experienced nurses (Delaney, 2003). This method of evaluating the performance of NGNs sees their work condemned as unsatisfactory and is often associated with stress among the new graduates joining the workforce.
Want help to write your Essay or Assignments? Click here
Control
Many NGNs report concerns about the control or autonomy of their new roles as practicing nurses. Many new nurses complained that being responsible and accountable to patients was stressing (Delaney, 2003). Duchscher and Cowin (2004) pointed out student nurse roles did little to equip NGNs for the responsibilities awaiting them in practice. Duchscher and Cowin (2004) support the view that patient care decision and outcome responsibilities often overwhelm new nurses.
However, the reactions of the NGNs varied as some embraced the new responsibilities, but most reported a feeling of being overwhelmed (Delaney, 2003). Researchers have argued that control is a double edged sword in the transition period. For nurses who embrace responsibility and accountability easily, it is exhilarating and exciting. In contrast, control brings about a feeling of anxiety for nurses who are unprepared for the new responsibilities.
NGNs may also suffer disorientation and poor sense of control as a result of unfamiliarity with the practice environment. NGNs are surprised when they realize that the practice environment is significantly different from the school context (Duchscher, 2001). Chang and Hancock (2003) argue that NGNs can experience as a result of uncertain expectation of the new role which gives rise to role ambiguity.
Support
Support by supervisors or coworkers plays a significant role in easing the NGN transition process. Often NGNs expend much effort in trying to familiarize themselves with existing workers in their healthcare setting (Casey et al, 2004). Duchscher and Cowin (2004) note that NGNs are in need the support of other members of the multidisciplinary team. Majority of NGNs report that there are adequately supported by preceptors and colleagues (Delaney, 2003).
They also reported that they felt part of the team. However, new nurse could not challenge established ways of doing things as they lacked support in doing this. Nurses also need support from family and friends outside the workplace. In fact, nurse reported that they performed better when they received support from outside the workplace.
Self-efficacy
Casey et al (2004) reported that NGNs feel incompetent and inadequate as they begin practicing as nurses. Many new nurses report feeling as if they did not posses the necessary skills or knowledge to work as Registered Nurses (Delaney, 2003; Duchscher and Cowin, 2004). NGNs also greatly doubted their clinical competence as they lacked a frame of reference unlike experienced healthcare workers (Duchscher and Cowin, 2004). Duchscher and Cowin (2004) points out those NGNs felt their inadequate knowledge was a serious limitation. However, NGNs reported higher self-efficacy and confidence scores as they continued to gain clinical experience.
Want help to write your Essay or Assignments? Click here
Transition Impacts
Job stress
Job stress is one of the most widely reported results of the NGN transition (Delaney, 2003; Duchscher and Cowin, 2004; Twibell et al 2012; Pellico, Brewer and Kovner, 2009). Despite the emphasis on job stress in many studies, few have investigated the intensity of stress affecting NGNs. Chang and Hancock (2003) reported that the transition experience resulted in moderate amounts of stress among NGNs. According to Casey et al (2004), NGNs comfort and confidence is initially very high as the new graduates join the profession, however, it decreases with time in the job.
Fortunately, nurse comfort and confidence starts to increase as they gain experience and peaks one year after commencing practice. Chang and Hancock (2003) reported that nurses experience many stressors during the transition process. According to the two, the initial stressors include role ambiguity and responsibilities. After one year of employment, the main stressor is role overload.
Job Satisfaction
One of the most ignored outcomes of NGN transition is the job satisfaction impact. Common studies have emphasized on the challenges experienced during the transition phase but rarely have the satisfying job aspects being explored. Delaney (2003) reported that some new nurses reported that they found their new roles as practicing nurses satisfying. Nurse’s satisfaction with their work increased when they started to recognize available opportunities for personal growth and development.
Some NGNs reported that it felt exciting to finally take up the role of a practicing nurse. However, NGNs also reported many dissatisfying elements in their work, these included dizzying pace of work, inadequate staffing and too much autonomy and responsibility (Pellico, Brewer and Kovner, 2009; Casey et al, 2004; Chang and Hancock, 2003). Nurse who were satisfied with their work also were also more intent on staying with their employer.
Further research explored job satisfaction as an independent variable and presented interesting research findings. Delaney (2003) reported that nurses who were satisfied with their jobs felt a strong sense of belonging to the organization. Satisfaction in jobs was also negatively associated with role stress, role ambiguity and conflict during the transition process (Chang & Hancock, 2003).
Research has also explored outcomes such as turnover intent and nurse turnover. Many of these outcomes increase when there is shortage of nursing manpower. A high patient:nurse turnover is likely to precede and increase in patient mortality and has been indicated as an accelerator of nurse burnout (Bowles and Candela, 2005). Nurses report that the main causes of high turnover among NGNs are poor work design and emotional exhaustion.
These result support the need to research into self-management strategies that nurses can use to cope to the stressing experiences of the transition process. Twibell et al (2012) have hypothesized that self-care strategies may help nurse achieve higher levels of satisfaction with their jobs.
Interventions to support NGNs
Decades of research have popularized the notion that NGN transition is a process that needs to be addressed (Bowles and Candela, 2005). Many interventions have been applied to assist is making the transitioning process easy. However, there are few reports of intervention that aim to teach nurses how to self-manage the transition by performing recommended self-care practices.
Early studies recommended the use of internship programs and preceptor pairing to expose the nurse to the “real world” prior to commencing practice (Bowles and Candela, 2005). However, the value of preceptor and internship programs have come into questions recently and new research is needed to clarify the value they add to the NGN transition process.
One of the gaps in NGN transition research is the lack of measurement of the effectiveness of interventions to support NGN transition (Bowles and Candela, 2005). Many of the early studies, presented subjective results of the effectiveness of the interventions they were studying. Later studies in the late 1980s started to include quantitative measures of the effectiveness of the interventions (Casey et al 2004). However, most of the studies failed to measure the impact of the studies on patient outcome. Some of these studies are included in this review.
Conclusion
The NGN transition process is a well researched area within the nursing profession. Most stakeholders seem to be aware of the problems that face NGNs as they transition into their practice. Decades of research present findings detailing mostly ineffective interventions to deal with the NGN transition process. One of the most common intervention experimented in research was the use of internship, residencies and preceptors. However, many researchers call into question the usefulness of these interventions in addressing the problems of new nurse’s commencing practice.
This research reveals two reasons why intervention to smooth the NGN transition failed to work despite decades of research. First, the early interventions were never objectively evaluated and thus the opportunity to gauge their effectiveness and increase their impact was missed. Furthermore, most of the intervention were designed to address problems identified in specific health care settings and were not backed by an understanding of the issues facing NGNs.
Few of the interventions sought to get to the bottom of the stress experienced by NGNs. Secondly, the interventions failed to take into consideration the many elements of the practice environment. This review presents some of the environmental factors that lead to a difficult experience for NGNs transitioning to practice. NGNs perception of their own abilities and knowledge is among the most stressing factors.
Many NGNs feel incompetent and inadequate when there are starting out. This attitude contrast sharply to the work demand, high expectation, and responsibility that characterize their work environment. Other healthcare workers expect nurses to exhibit the same level of competence and skills as experienced practitioners less than two months after being employed.
Few nurses are prepared for the sudden responsibility and autonomy they have over patient care decision. Many find the new responsibility overwhelming and are stressed. However, a substantial number of new nurses are excited and exhilarated to work autonomously. This review also indicates that support from colleagues, supervisors, family and friends are important for a successful transition. Nurses who receive support express confidence in their ability, Skills and knowledge.
This review has revealed that the NGN transition process can be an extremely stressing period. Many studies point to the stress and emotional distraught that is experienced by NGNs during the transition. Most studies report that new nurse feel overwhelmed by the demands of the new environment, feelings of inadequacy and fear of failure. Very few studies have investigated the possible positive impact of self-care mechanism that may assist nurse’s cope with the difficult transition period. This research will seek to address this gap in research and provide valuable evidence that may be used to improve the NGN transition experience significantly.
References
Bowles, C., & Candela, L. (2005). The first job experiences of recent RN graduates. Journal of Nursing Administration, 32(3), 130Y136.
Casey, K., Fink, R. R., Krugman, A. M., & Propst, F. J. (2004). The graduate nurse experience. Journal of Nursing Administration, 34(6), 303-311.
Chang, E., & Hancock, K. (2003). Role stress and role ambiguity in new nursing graduates in Australia. Nursing & health sciences, 5(2), 155-163.
Cho, J., Laschinger, H., & Wong, C. (2006). Workplace empowerment, work engagement and organizational commitment of the new graduate nurses. Nursing Leadership, 19(3), 43Y60.
Duchscher, J. E. B., & Cowin, L. S. (2004). The experience of marginalization in new nursing graduates. Nursing Outlook, 52(6), 289-296.
Dyess, S. M., & Sherman, R. O. (2009). The first year of practice: New graduate nurses’ transition and learning needs. The Journal of Continuing Education in Nursing, 40(9), 403-410.
Edwards, D., Hawker, C., Carrier, J., & Rees, C. (2015). A systematic review of the effectiveness of strategies and interventions to improve the transition from student to newly qualified nurse.International journal of nursing studies, 52(7), 1254-1268.
Halfer, D., & Graf, E. (2006). Graduate nurse perceptions of the work experience. Nursing Economics, 24(3), 150.
Pellico, L. H., Brewer, C. S., & Kovner, C. T. (2009). What newly licensed registered nurses have to say about their first experiences.Nursing outlook, 57(4), 194-203.
Romyn, D. M., Linton, N., Giblin, C., Hendrickson, B., Houger Limacher, L., Murray, C., … & Weidner, A. (2009). Successful transition of the new graduate nurse. International Journal of Nursing Education Scholarship, 6(1).
Scott, E. S., Engelke, M. K., & Swanson, M. (2008). New graduate nurse transitioning: necessary or nice?. Applied Nursing Research,21(2), 75-83.
Twibell, R., St Pierre, J., Johnson, D., Barton, D., Davis, C., Kidd, M., & Rook, G. (2012). Tripping over the welcome mat: Why new nurses don’t stay and what the evidence says we can do about it. American Nurse Today, 7(6), 357-365.
Waite, R. (2004). Psychiatric nurses: Transitioning from student to advance beginner RN. Journal of the American Psychiatric Nurses Association, 10(4), 173-180.
Want help to write your Essay or Assignments? Click here
Want help to write your Essay or Assignments? Click here
Identifying a Problem
The diagnosis and management of depression within the American population remains one of the health factors affecting the health sector. Sources determine that the prevalence of depression within the American population is ascertained to stand at 8.5%, a factor that has seen less people seek medical attention (Wagner, Müller, Helmreich, Huss, & Tadić, 2015). Thus paper therefore seeks to develop a PICOT question in determine the aspect of depression and its effects within this population.
PICOT Question
It is essential to consider that the PICOT P, Population: I Intervention C, Comparison, O, Outcome and T Time is developed in guiding this study. In the American population between the ages of 30-35 of the working class (P), is there a need of developing a tool that will analyze depression (I), compared with the other approaches of care (C) that ensures appropriate procedures are developed in order to detect depression (O) within a specified time (T)? The aim of the PICOT question is developed to determine enough evidences that justify the element of depression among the American population through the use of effective tools.
Selecting Sources of Literature
In considering the results of this paper, it is essential to search through multiple databases that include EBSCOhost, Google Scholar, PsycINFO and the Cochrane and other sources from Health Care research centers. In getting the results of this study, there are key search words that need to be considered (Wagner, et.al.2015). These words include: screening, depression, depressive disorders, BECK or BDI-ii and the population. The use of both the published and the unpublished materials in searching the literatures was incorporated with the materials reviewed dating back between 2005-2010.
Selecting Sources of Literature
According to Wagner et.al.2015, a metal-analysis was conducted to determine the effects of depression on the American population. The findings of the study identifies that a majority of the population presented traumatic symptoms. This material determines that depressive disorders among the younger generation may lead to suicidal and homicidal thoughts and attempts (Jackson, Dianne & Garnefski, 2015).
Some of the symptoms that are presented by this author include chest pains, headaches, painful urination, dizziness an excessive sweating. This source intrinsically supports the specified area of study since it provides evidence to some of the effects of depression among the American population.
Want help to write your Essay or Assignments? Click here
Jackson et.al.2015 in his literature consequently revealed that the screening of depression among the American population undergoes a process of identification, assessment, and initiation of approaches aimed at managing this disease within the American population (pp.197). This author details a quantitative randomized study within this population and establishes that the abuse of substances is as a result of depression, a factor that explains the reasons why several Americans engage in risky sexual behaviors.
On the other hand, the population is also likely to engage in drugs and substance abuse as a result of depression. The author determines that there is a need of developing a concurrent treatment method that uses psychotropic drugs and other stable stimulants in the management of depression. The inclusion of psychotherapeutic method is also essential in the management of depression.
The author also mentions that depression within this population needs to be effectively managed since discoveries have been made that establish individuals in this state engage in unprotected sex and the inclusion of multiple sexual partners, a factor that would result into a health concern within a nation.
References
Wagner, S., Müller, C., Helmreich, I., Huss, M., & Tadić, A. (2015). A meta-analysis of cognitive functions in children, adults and adolescents with major depressive disorder. European Child & Adolescent Psychiatry, 24(1), 5-19. doi:10.1007/s00787-014-0559
Want help to write your Essay or Assignments? Click here
Diabetes Mellitus
Being newly diagnosed with diabetes mellitus can be overwhelming and confusing due to the several things that a patient needs to learn and understand. However, for millions of diabetic patients learning about their diabetes is the first step towards living a longer and healthier life. According to Shaw (2014), Registered Nurses (RNs) play an important role of educating individuals that have just been diagnosed with diabetes mellitus encouraging them that they can live longer if they follow important guidelines for managing diabetes.
First, the RN should let the patient understand what type 1 diabetes is and how its symptoms present by highlighting the classic symptoms associated with diabetes mellitus such as excessive thirst and hunger, fatigue, unexplained weight loss, nausea, and vomiting. She should encourage the patient that he is not the only one suffering from type I diabetes.
Most youth with type 1 diabetes do not adhere to clinical guidelines (Wood et al, 2013). Therefore, the nurse can use examples of patients of almost similar age to the patient and are coping well with diabetes mellitus. The nurses should also explain to the patient that insulin injections are the central treatment for type I diabetes and for the patient to lead a quality life she should adhere to her medication.
For proper management of type I diabetes, some of the factors that the RN should focus on mainly includes control of blood glucose, insulin management, nutrition, exercise, and support (Atkinson, Eisenbarth & Michels, 2014). The nurse should advise the patient to measure his blood glucose levels regularly and administer insulin appropriately. Exercise on the other hand is a significant component of proper care for type I diabetes as it aids the body to respond with more stable levels of blood glucose (Haas et al., 2013).
Want help to write your Essay or Assignments? Click here
However, patients should be cautioned against extreme exercise which lowers their glucose levels considerably. Additionally, the nurse should aid the patient understand how various foods affect blood glucose and enlighten them on how to come up with solid meal plans (Chiang et al., 2014). She should also encourage the patient to seek help from other people with the same condition and be free to visit the medical center in case of any clarification.
The steps of the teaching learning process that were most likely not well employed are the implementation and the evaluation steps. In the implementation step, the nurse should have delivered content in a manner that is more organized with the aid of planned teaching strategies. The evaluation step could be improved if the nurse questioned the patient on some aspects such as why insulin is important in management of type I diabetes and more so the rationale of giving it as an injection instead of pills.
References
Atkinson, M. A., Eisenbarth, G. S., & Michels, A. W. (2014). Type 1 diabetes. The Lancet, 383(9911), 69-82.
Chiang, J. L., Kirkman, M. S., Laffel, L. M., & Peters, A. L. (2014). Type 1 diabetes through the life span: A position statement of the American Diabetes Association. Diabetes Care, 37(7), 2034-2054.
Haas, L., Maryniuk, M., Beck, J., Cox, C. E., Duker, P., Edwards, L., … & McLaughlin, S. (2013). National standards for diabetes self-management education and support. Diabetes care, 36(Supplement 1), S100-S108.
Shaw, R. J., McDuffie, J. R., Hendrix, C. C., Edie, A., Lindsey-Davis, L., Nagi, A., … & Williams, J. W. (2014). Effects of nurse-managed protocols in the outpatient management of adults with chronic conditions: a systematic review and meta-analysis. Annals of internal medicine, 161(2), 113-121.
Wood, J. R., Miller, K. M., Maahs, D. M., Beck, R. W., DiMeglio, L. A., Libman, I. M., … & T1D Exchange Clinic Network. (2013). Most youth with type 1 diabetes in the T1D Exchange Clinic Registry do not meet American Diabetes Association or International Society for Pediatric and Adolescent Diabetes clinical guidelines. Diabetes care, 36(7), 2035-2037.
Want help to write your Essay or Assignments? Click here