Want help to write your Essay or Assignments? Click here
The diagnosis and management of depression within the American population
Identifying a Problem
The diagnosis and management of depression within the American population remains one of the health factors affecting the health sector. Sources determine that the prevalence of depression within the American population is ascertained to stand at 8.5%, a factor that has seen less people seek medical attention (Wagner, Müller, Helmreich, Huss, & Tadić, 2015). Thus paper therefore seeks to develop a PICOT question in determine the aspect of depression and its effects within this population.
PICOT Question
It is essential to consider that the PICOT P, Population: I Intervention C, Comparison, O, Outcome and T Time is developed in guiding this study. In the American population between the ages of 30-35 of the working class (P), is there a need of developing a tool that will analyze depression (I), compared with the other approaches of care (C) that ensures appropriate procedures are developed in order to detect depression (O) within a specified time (T)? The aim of the PICOT question is developed to determine enough evidences that justify the element of depression among the American population through the use of effective tools.
Selecting Sources of Literature
In considering the results of this paper, it is essential to search through multiple databases that include EBSCOhost, Google Scholar, PsycINFO and the Cochrane and other sources from Health Care research centers. In getting the results of this study, there are key search words that need to be considered (Wagner, et.al.2015). These words include: screening, depression, depressive disorders, BECK or BDI-ii and the population. The use of both the published and the unpublished materials in searching the literatures was incorporated with the materials reviewed dating back between 2005-2010.
Want help to write your Essay or Assignments? Click here
Selecting Sources of Literature
According to Wagner et.al.2015, a metal-analysis was conducted to determine the effects of depression on the American population. The findings of the study identifies that a majority of the population presented traumatic symptoms. This material determines that depressive disorders among the younger generation may lead to suicidal and homicidal thoughts and attempts (Jackson, Dianne & Garnefski, 2015).
Some of the symptoms that are presented by this author include chest pains, headaches, painful urination, dizziness an excessive sweating. This source intrinsically supports the specified area of study since it provides evidence to some of the effects of depression among the American population.
Jackson et.al.2015 in his literature consequently revealed that the screening of depressive disorders among the American population undergoes a process of identification, assessment, and initiation of approaches aimed at managing this disease within the American population (pp.197). This author details a quantitative randomized study within this population and establishes that the abuse of substances is as a result of depression, a factor that explains the reasons why several Americans engage in risky sexual behaviors.
On the other hand, the population is also likely to engage in drugs and substance abuse as a result of depression. The author determines that there is a need of developing a concurrent treatment method that uses psychotropic drugs and other stable stimulants in the management of depression. The inclusion of psychotherapeutic method is also essential in the management of depression.
The author also mentions that depression within this population needs to be effectively managed since discoveries have been made that establish individuals in this state engage in unprotected sex and the inclusion of multiple sexual partners, a factor that would result into a health concern within a nation.
References
Wagner, S., Müller, C., Helmreich, I., Huss, M., & Tadić, A. (2015). A meta-analysis of cognitive functions in children, adults and adolescents with major depressive disorder. European Child & Adolescent Psychiatry, 24(1), 5-19. doi:10.1007/s00787-014-0559
Want help to write your Essay or Assignments? Click here
Beck’s Cognitive Theory of Depression: Incorporating Theory
Description
For the proposed research, the PICO question that guides the study is as follows: In young adults aged 30 to 35 years-old (P), is using a screening tool for depression (I), in comparison to the usual standard of care (C), more accurate in detecting depression (O). This PICO question helps in finding out whether or not there is sufficient evidence to support screening young adults aged 30 years to 35 years for depression with the use of a suitable screening tool.
Utilization in Supporting Solution
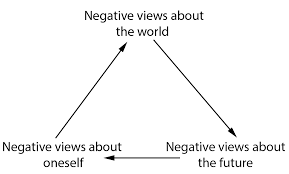
The theory that could be utilized in supporting the proposed solution is Beck’s Cognitive Theory of Depression. Beck identified 3 main components or mechanisms which are responsible for depression. These include: (i) negative self schemas; (ii) the cognitive triad; and (iii) errors in logic, that is, faulty processing of information (Abela & D’Allesandro, 2012). The cognitive triad are 3 types of negative thinking which are common in people who have depression: that is negative thoughts concerning the future, the world, and the self.
These negative thoughts are automatic in individuals with depression since they occur impulsively. Beck pointed out that people who are prone to depression develop a negative self-schema. Such an individual possesses various expectations and beliefs regarding himself or herself which are pessimistic and negative. Individuals who have negative self schemas are inclined to making logical errors in their thinking. They are also inclined to focusing mainly on particular facets of a situation whilst disregarding other information that is equally pertinent (Abela & D’Allesandro, 2012).
Want help to write your Essay or Assignments? Click here
The rationale for selecting this theory is that this theory helps to describe what really is central to depression; that is, the main cause of depression. According to Beck, the cognitive symptoms of depression in fact precede the mood and affective symptoms of depression, and not the other way round. What is central to depression, as Beck pointed out, are the negative thoughts and not low reinforcement rates or hormonal changes as other theorists had suggested (Abela & D’Allesandro, 2012).
This theory works to support the proposed solution in that using depression screening tools, the researcher will be able to determine more accurately the main cause of depression amongst young adults in the United States. In other words, using appropriate screening tools for depression, it would be possible to detect the negative thoughts in people aged 30-35 in the United States considering that negative thoughts are central to depression as per Beck’s Cognitive Theory of Depression.
Incorporation
The theory would be incorporated into the project by using screening tools for depression which are in line with Beck’s Cognitive Theory of Depression. One particular screening tool that would be used is the Beck Depression Inventory-II (BDI-II) which was developed by the same theorist who conceptualized Beck’s Cognitive Theory of Depression. The BDI-II screening tool for depression would be utilized to detect depression among 30-35 year-old young adults and it would be compared with the usual standard of care currently being practiced in the country.
In essence, using Beck’s Cognitive Theory of Depression, the negative thoughts of people would be carefully monitored using Beck Depression Inventory. It is expected that depressed people negatively misunderstand information and experiences, as they limit their focus to the negative facets of a situation, therefore feeling hopeless regarding the future (Abela & D’Allesandro, 2012). Using Beck’s Cognitive Theory of Depression in the project, a direct correlation is postulated between severity of symptoms of depression and negative thoughts.
Want help to write your Essay or Assignments? Click here
Child Development Theory and Practices
Introduction
Childhood development is the theory and practice of procedures to ensure that the child is given the proper resources, guidance and nutrition to see them through their infancy up to middle school. Child development can also be the biological, social and psychological change in a child as they grow. However, it is supported by the various efforts and developmental models chosen and taken by their parents and guardians. Indeed, the development of a child involves aspects such as pedagogical development and the development of the various biological systems in the body.
The whole process is geared towards achieving total autonomy in the child. Children are exposed to many issues at an infant age. The most challenging of these issues is the introduction of new diet. Children often have to begin feeding on supplementary diet that is different from mammary milk after they attain the age of twelve months. Child development policies and strategies ensure that these steps and stages in the development of the child are done incrementally and professionally to achieve desired impact (Bevans, Riley & Forrest, 2010).
Background on child development
Child development has been a source of scientific and medical research over the last few decades. Policies in child development often relate to the ability of the parent to help them achieve autonomy. However, with regard to theories in child development, the concern has often been about the emotional and physical relationship of the child and the mother. Many studies have been done on issues in child development. They have since resulted in aspects of child treatment, immunization and even nutrition.
The most significant theories in child development are the Developmental theories and the attachment theories (Warner, 2007). It is necessary however to realize that although most of the theories on child development have hardly been refuted, they have not been unanimously approved as well. Child development is often the cause of controversy in many policy development forums. There are particular goals that need to be achieved in child development but many different approaches to achieve these theories.
Where child development in a biological context is concerned, the physical change in the body of a child as they move from childhood to puberty is often a marvel in scientific research. Many children often realize a particular affinity for certain objects, games and pleasantries as they grow. However, there is likely that a child’s growth potential is achieved by the time they reach puberty (Bevans, Riley & Forrest, 2010). Children however do not easily learn the psychomotor skills on their own.
The exposure the child gets as they grow often determines how well they grow with regard to psychological and emotional development. There is indeed a direct relationship between the child’s environment and their eventual personality traits. More so, the adaptability of the child at the infancy stage is higher than at any other stages in their development. This is why child development theory and practice takes center stage among many pediatric research and education practices (Capel, 2012).
Child development however exceeds past growth. For instance, when a child grows, organs do not just grow, they are specialized. The same is the case for the various body cells and senses. They become bigger (grow) and better at their functions (develop). Child development theories thus take all these issues into account. However, with regard to the aspects and determining factors in child development; it is often the case that cases of child development complications are often treatable.
Medical research asserts that since the mind of the child keeps changing and growing, it is often the case that children may outgrow behavioral and psychological issues. There is however contention on the possibility of child brain research towards the treatment of regressive growth involving limbs and other bodily organs with a rich nervous system (O’Connor & McCartney, 2007).
Child Development Theories
Child development theories assess the growth and development of the child; the mitigating factors and the various aspects of the growth. Theories try and explain why phenomena such as development of limbs, ability to walk, talk and read as well as the growth of the intuition in a child occurs as it does. The major categories children are classified into often include; newborns, infants, toddlers, preschoolers, school-aged children and adolescents. These different categories of children often exhibit different traits.
This is why models are often specific to the category and explain how growth takes place from one category to the next. There are various theories formulated towards contributing to child development policies. However, this paper will discuss two main theories; child development theories and child attachment theories. These theories help scientists assess various growth factors and inhibitors to proper development of the child (Rigby, 2007).
Child development theories assess and explain the factors behind a child’s development. The most common of these theories is the ecological systems theory. The ecological systems theory was first proposed by Urie Bronfenbrenner. He proposed four categories for child biological development. These include; microsystem, mesosystem, exosystem and macrosystem. The microsystem of the child is the nervous and cardio vascular system. The mesosystem defines the muscular system in the body.
The exosystem defines the skin organ of the body and all systems that interact with the external environment while the macrosystem defines the organ system in the body. A child’s development is expected to take place simultaneously in all these four stages. The theory also proposes that each of these subsystems contains particular norms and principles that guarantee development in a symbiotic manner. The relationship between the systems defines how well or retarded growth in a child is.
The child attachment theory defines the psychological, evolutionary and ethological development of a child. The theory asserts that interpersonal relationships between human beings are based on the development and proliferation of psychological needs. These needs stem from the child’s emotional upbringing and contact with the environment they live in. It is thus a concern that needs to be addressed by care givers.
The child’s evolutionary needs have to do with the child’s nutrition and socialization. Aspects such as early schooling, introduction to sporting activities and involvement in household chores contribute greatly to child development. It is thus critical to achieve these early. However, ethological (behavioral) growth in a child is cultured from the observations the children make on their own. This is why the environment one raises a child in must be protected from unnecessary exposure.
Want help to write your Essay or Assignments? Click here
Early Childhood Education Theories
Early childhood education theories discuss the development of the child as they progress through school from introduction to later stages in school. For instance; the Development Integration Approach in child development discusses child development on aspects such as; physical, social, emotional, language and cognitive skills. Physical development is assessed through measures such as the body mass index (BMI) that evaluates the mass against the height of the child. Social and emotional development skills are the skills the child acquires from interacting with other children and adults.
Language can be considered in two aspects; the first language the child was exposed to; known as L1 and the other languages follow as L2, L3…However, language can also be the ability of the child to learn etiquette, euphemism and other necessary language skills at an early age. Cognition in a child is the most observable change. Abilities such as reading, learning and concentrating however take time to develop in a child. The ability to use language properly is very important to the child’s growth as it makes them able to communicate (Warner, 2007).
The other common theory in early childhood education is the socio-cultural learning theory. This theory asserts that the impact of the child’s social experiences as well as their cultural disposition affects their individual thinking and the development of their mental processes. This is why it is important to raise children in environments that elicit such growth potential.
All the same, whatever environment the child finds themselves in is able to affect their mental and psychological health either positively or negatively. The theory by Lev Vygotsky proposes that cognition should be trained by the child’s care givers since it occurs on a social context. Allowing children to play and undertake certain responsibilities early prepares them for such responsibilities in the future (O’Connor & McCartney, 2007).
For instance, early driving classes make the child develop an intuitive sense that helps them discern the path to take while on the road and the decisions that can help them avoid accidents and dangerous driving. Socio-cultural learning also presents the argument that a child born in cultural practices will likely learn them and embrace them early if they are exposed to them from the onset.
Conclusion
Early childhood development is a phenomenon that has been observed by scientists across the world for centuries. Indeed, aspects of child development such as the development of psychomotor skills, cognitive development and physical development often relate to the child’s culturalization. Most care givers are advised to monitor the path through which the child takes in their development actualization pattern in order to grow into the anticipated adults society envisions.
However, there are biological factors in child development and growth that do not really have anything to do with the care givers but actual parents. Genetic factors are often difficult to deal with as they are as the result of recessive genes since childhood. In such cases that these recessive genes lead to visible impaired limbs, it is necessary to seek medical attention to know how to handle these cases (Ogunnaike, 2015). Children should always be brought up in environments where they feel safe and able to interact freely with all persons in their vicinity. Since most of what they learn is acquired from vision, it is important to invest on the child’s environment and control it as much as possible without interfering with it.
References
Bevans, K. B., Riley, A. W., & Forrest, C. B. (2010). Development of the healthy pathways child-report scales. Quality of Life Research, 19(8), 1195-214.
Capel, C. M. (2012). Mindlessness/mindfulness, classroom practices and quality of early childhood education. The International Journal of Quality & Reliability Management, 29(6), 666-680.
Rigby, E. (2007). Same policy area, different politics: How characteristics of policy tools alter the determinants of early childhood education policy. Policy Studies Journal, 35(4), 653-669.
O’Connor, E., & McCartney, K. (2007). Examining teacher-child relationships and achievement as part of an ecological model of development. American Educational Research Journal, 44(2), 340-369.
Ogunnaike, Y. A. (2015). Early Childhood Education and Human Factor: Connecting Theories and Perspectives. Review Of Human Factor Studies, 21(1), 9-26.
An individual experiencing sensory impairment may face quite a number of challenges in life. With respect to higher level needs that are defined in Maslow’s hierarchy of needs. A visually challenged individual may find it harder to actualize these higher level needs. The higher level needs that include self-actualization, self-esteem and love and belonging needs, are among the particular needs that this paper will try to elaborate on how challenging they are to a visually challenged individual to meet them.
Love and belonging is nature to most if not all human beings. These needs depict the nature of the interpersonal relationships that are adopted by most humans. However, for a Sensory Impairment person. It may be quite difficult for them to find a sense of belonging in an environment that does not favor him or her. Creating interpersonal relationships with people without actually seeing their physical appearance will be the main issue to be dealt with.
Consequently, self-esteem needs are quite important in Maslow’s hierarchy. But for a Sensory Impairment person, attaining this needs may be a challenge. They may find it extremely hard to gain confidence. It might be quite difficult for this particular individual to be able to satisfy his or her desire to be valued by other people when he or she is visually challenged.
Lastly, self-actualization needs is on the pinnacle of Maslow’s hierarchy. Self-actualization entails five key things that are key to human beings. However, for visually challenged individuals, to fully satisfy their self-actualization need may prove to be hard if the person has not yet accepted the impairment condition that faces him or her.
The nursing intervention that would be applied by a registered nurse may include the following practices. First of all when meeting the patient, the nurse will have to make a good first impression. Reason being first impression go a long way into helping visually impaired patients feel cared for.
This also helps in creating a healthy relationship between the two parties (Treas & Wilkinson, 2013). Second of all, the nurse would help the patient meet their self-esteem and self-actualization goals by helping then get to know the environment they are staying in. This would help them feel confident by not requiring aid all the time to perform the basic life activities from time to time.
Therefore, for a visually impaired individual, the attainment of the love and belonging, self-esteem and self-actualization goals may be a cumbersome task. However, with the application of the right nursing intervention by a registered nurse. The attainment of these needs in the long run may be an overcome able situation.
Improving mental health efficiency by using of community health workers to decentralize health care services
Overview of healthcare industry, markets and competition
Recent changes in the UK in National mental Healthcare Services (NHS) have introduced new complexities into the accountability arrangements of the healthcare facilities. The current mental health systems are best described as command and control system. The mental budgets as well as policy are strategically set centrally by the Department of Health (DoH) and the government is administered locally by the NHS organization but accountability lies with the DOH.
The situation is more complex than the explanation of the ‘command and control.’ The balances between the central government and the local government have led to fluctuating autonomy and misallocation of resources (Normand, 2011).
The UK mental healthcare system relies on highly centralized and costly expertise to delivery healthcare services. This type of system relies in intuitive medicine, and is best suited for healthcare issues that are complex and episodic. In addition, this type of healthcare system is associated with mismatch for chronic diseases, preventive measures and wellness care; which results into additional barriers and disparities especially among the underrepresented population.
It is time for the National Health System (NHS) to depart from a one-size-fits all model and develop channels that will enable better delivery of services that can serve the dynamic needs of the population (Clayton, 2009).
This study proposes that decentralizing mental healthcare services will aid in lowering cost of care, broaden accessibility and maintain as well as improve quality of care. For instance, the physician specialist will have the capacity to work in outpatient, the nurse practitioner will effectively provide care in retail clinics, and lay community health promoters or workers will improve health education, thereby reducing health complications associated with disease progression.
For example, the system will improve diabetic self management at patient’s residents. This measure is in line with Institute of Medicine (IOM’s) health disparity vision of confronting ethnic and racial disparities using strategies that improve care delivery and or implement preventive measures and to enhance risk reduction (Black & Gruen, 2005).
Perceived problems in current healthcare systems
The fundamental issue that is believed to affect mental healthcare activities includes quality of care, safety issues, access to healthcare, cost of care, and delivery of services. These issues arise because of the problems that affect healthcare systems which include misallocations of national health resources, allocative inefficiency, and increased inequalities. Most of the health facilities get less proportion of healthcare budgets. An example of healthcare system that suffers from misallocation of resources is the mental healthcare system, which suffers due to misallocation of resources within the sector (Goodwin, Gruen, & Iles, 2006).
In my facility, funding is done on low cost effective-interventions such as non-essential prevention strategies. For instance, People diagnosed with substance use along with mental health (commonly referred to as dual diagnosis) is associated with many health demands, yet they suffer too much to access quality healthcare services. These patients have complex needs and often experience multiple adversities in their lives including deprivation, childhood abuse, poverty and loss of support from their family members.
These persons are also associated with multiple needs such as homelessness and unemployment that makes them become prone of exploitation. This increases their risk of poor physical health, self harm, suicide and perpetrating violence. Dual diagnosis is unpopular in the UK, partly because the society is entrenched perceptions of substance abuse where most people believe that is a lifestyle choice instead of a health issue that needs urgent care and treatment (Normand, 2011).
Dual diagnosis is one of the issue facing mental health and substance abuse. In the past one and half decades has lead to development of specific initiatives but all of them have had no improvement. The same changes have been implemented since the 90s. Today, mental health services today still exclude people if the problem is not perceived as substance related disorders. The misallocation of resources is associated with inefficient delivery of care as most of the healthcare resources are wasted (Kirk and Glendinning, 1998).
For example, it is inefficient to give patient a brand name over drugs cheaper generic ones that have same efficacy. The misallocation of resources also results to underutilization of resources which also affects the productivity efficiency. In current type of healthcare system often leads to indiscretions such as specialists handling numerous uncomplicated cases at high cost, cases that primary care centers could handle with ease (Normand, 2011).
The aforementioned factors have lead to increase on cost of care without matching consumer’s health benefit. In addition, the existing weak monitoring system enables leakages of public subsidies to private sectors and medical covers which are already financially stable. This results to increased health disparities where poor and under-privileged in the society lack care affordability (World Health Organization, 2000).
These affected populations unfortunately are the majority, and often receives low quality of care. One of the best strategies is to train the staff in mental health facility in order to equip them with skills that will help make dual diagnosis by improving their knowledge and skills but have not managed to change the society’s perception and values.
Therefore, the two great challenges in this aspect of mental health a) to increase awareness on dual diagnosis in order to change attitudes people’s attitudes on mental health and b) to provide effective services to people diagnosed with dual diagnosis, especially in this unprecedented mental health crisis (Normand, 2011).
Change in mental healthcare systems
Change in the healthcare system is intended to improve the performance by adjusting the way services are delivered and relocating or roles and responsibilities for specific healthcare services and the processes of delivering care to the population including financing, implementation process, monitoring as well as regulation. There are various drivers of change in the current health care system including the expected shift in political, social and economic factors that will come with new governing system. In addition, the increase in technological advancement should be enhanced to not only improve quality of care, but also the accessibility (Normand, 2011).
The key drivers for the proposed change within the mental healthcare system in NHS includes changes in population growth, demographic characteristics due to immigration, technological advancement, health’s infrastructure conditions, and increased patient level of acuity. Change in ideologies refers to the modifications of frameworks used by the public health services to deliver care. For instance, new labor in 1997 removed department of health monopoly which created more opportunities for private sector and voluntary services that helped better healthcare system to some extent, at higher cost of care.
Similar changes have been observed with the coalition government in 2009 which removed government agents and gave more roles to local authorities and the private providers, which led to increase misallocation of resources. Therefore, decentralizing delivery of healthcare services using community workers will create freedom for providers to innovate strategic services that meet the specific demands for patient needs (Pickard and Glendinning, 2002).
In addition, the current infrastructure conditions are too old and are not adaptable to provision of modern care for dual diagnosis. The current healthcare infrastructure demerits include high cost of care, reduced staff retention and inconsistencies in delivery of care. Therefore, vertical integration of decentralized health care in this community is aimed at addressing these challenges by reconfiguring healthcare services to suit the specific community demands.
For instance, technological advancement has made it easy to access patient information and also increased portability of patient’s health information and education of appropriate optional treatment. It is time to tap on the innovative techniques to increase efficiency in delivery of mental healthcare system and manage delivery of care in a way that maximizes population health benefits (Duguid & Pawson, 1998).
Changes in population growth and the demographic factors is also another driving force for decentralization of mental healthcare services by the NHS. The increase in population has put pressure on the current healthcare system as it has led to dilapidation of healthcare facility caused by congestion due to population growth, which has led into high demands building of bigger healthcare facilities that will accommodate the patients.
In addition, the gentrification of the low socioeconomic households by the middle class has led to inconsistence in delivery of services. The increased patient level of acuity and knowledge on quality issues is pushing the healthcare providers to improve delivery of care in order to meet their expectations (Clayton, 2009).
Recommendation
Change refers to any alteration of healthcare services with the aim of improving its quality. Changes in healthcare system are wide and ranges from revolutionary technology to refining of health workers responsibilities. There are three types of change namely originates, borrowed and adapted. Borrowed changes are easy and cheap to implement. However, these types of changes are often not appropriate to meet the local needs as no community is similar to another, which implies that one size fits to all may not apply (Goodwin, Gruen, & Iles, 2006).
The proposed change is adapted change, which mainly implies that the strategies are borrowed from elsewhere and gets modified to fit the community needs. However, factors such as situational circumstances, management approach, wrong adaptation, and changes in political as well as economic environments determines if the change process will be effective or not.
Originated changes would be more effective as it involves more creativity than the adapted changes, but their implementation process is expensive as it requires an organizational climate that promotes innovation and creativity. The proposed change is a technical change as it modifies the ways in which normal activities are carried out by altering the organization and program structures (Clayton, 2009).
Decentralization is kind of change that involves dispersal of administrative, political and financial functions. It involves a process of shifting authority, power and responsibility from national to local government levels of the healthcare systems. The main advantages for vertical integration of decentralization in mental healthcare system includes technical benefits such as improving delivery of healthcare services, leading to better health outcomes. In addition, this method eradicates challenges associated with bureaucracy and monopoly that hinders effective delivery of healthcare services to the needy service users (Atun, 2007).
Political benefits associated with decentralization of healthcare services are that it extends democratic control of healthcare services to the needy individuals at community level. This may also increase opportunity for the citizens and services users to participate in decision making processes. This is effective strategy as it helps the government to identify the specific community needs.
Decentralization process also helps in minimizing financial burden associated with public procurement processes by transferring risks from a central point and distributing them to lower and private sector. This helps promote innovativeness and competition, which further improves the service user’s outcome (Bossert, 1998).
In this context, decentralization is the recommended as an approach of improving administrative activities that will help deliver healthcare services. This is also done for the purposes of achieving effective service delivery. In addition, decentralization helps improve local participation as well as autonomy in healthcare services. This acts as a means of redistributing power when it is effectively done, thereby reducing health disparities associated with tribal and regional tensions.
Decentralization is also invoked as a means of increasing cost efficiency in mental health care systems, which is attained by giving the local units better and greater control over the available resources as well as healthcare revenues. In turn, this approach sharpens NHS accountability in healthcare services and operations. The approach helps to covertly offload financial burden from resource poor governments to local service providers (Saltman et al., 2007).
Conclusion
The Mental healthcare system relies upon on highly centralized and costly. The optimal for mental healthcare system is based on intuitive medicine, and is best suited for complex and episodic mental health complication. This increases additional barriers to healthcare care disparities and the minority groups. It is important for the NHS mental health care system to depart from the one size fits all paradigms and to establish better channels that will ensure that healthcare delivery is improved to meet the growing dynamic needs for the underprivileged service users.
The potential impacts of decentralization intervention are that it creates opportunities that improve the prevention strategies. The balance between the primary and tertiary preventive measures regarding saving. The strategy will also increase access to healthcare services by ensuring that the downstream expenses are balanced. In addition, the approach will help replace the costly unnecessary services with less expensive and quality ones.
References
Atun, R. (2007). Privatisation as decentralization strategy, Chapter 14, 247-266. In Saltman, R. B., Bankauskaite, V., & Vrangbaek, K. Decentralization in Healthcare. European Observatory on Health Systems and Policies Series. McGraw Hill, Open University Press. Maidenhead, Berkshire, England.
Black, N., & Gruen, R. (2005). Understanding Health Services. Open University Press, Berkshire, England
Clayton, M. (2009). The Management Models Pocketbook. Management Pocketbooks
Duguid, S. & Pawson, R. (1998). Education, change and transformation: The prison experience. Evaluation Review. 22(4), 470-95
Goodwin, N., Gruen, R., & Iles, V. (2006). Managing Health Services: Understanding Public Health. Open University Press, Berkshire, England
Kirk, S and Glendinning, C. (1998). Trends in community care and patient participation: implications for the roles of informal carers and community nurses in the United Kingdom. Journal of Advanced Nursing 28:370-81
Normand, C. (2011). The healthcare system in Ireland: Controlling growth in expenditure and making best use of resources. Chapter 3 (pp 57-74). In Callan, T. (editor). Budget Perspectives 2012. Economic & Social Research Institute (ESRI) Research Series 22, Dublin.
Pickard, S and Glendinning, C. (2002). Comparing and contrasting the role of family carers and nurses in the domestic health care of frail older people. Health and Social Care in the Community 10: 144-50
Saltman, R. B., Bankauskaite, V., and Vrangbaek, K. (2007). Decentralization in Healthcare. European Observatory on Health Systems and Policies Series. McGraw Hill: Open University Press.
World Health Organization (2000). The World Health Report 2000. Health Systems: Improving Performance, WHO, Geneva.
Want help to write your Essay or Assignments? Click here
About 1 percent of the entire population has intellectual disability, which is a considerable disorder in adaptive as well as intellectual function in the early stages of development (Aveyard 2014). Individuals with the intellectual disabilities rate of developing mental illness are greater in comparison to the whole population, however, challenges in communication, access to services, literacy means that mental issues in persons with intellectual disability are inadequately recorded.
Moreover, the majority of persons with intellectual disability exhibit challenging behaviors, meaning characters of intensity, duration, and frequency that endangers their physical safety or those around them or even restricts accessing community services.
For a long period, there have been concerns that psychotropic medicine especially, antipsychotics are overused as such prescribed for problem behavior instead of diagnosing mental sickness, regardless of insufficient proof on their effectiveness. Nonetheless, getting an accurate amount of psychotropic in persons with learning disabilities is intricate, while present literature is limited due to varying descriptions.
In spite of inadequate proof from policy context, there is no detailed assessment of psychotropic in adults with learning disability in United Kingdom primary care conducted, while results from other nations cannot be generalised due to variations in health care provisions as well as practices (Guerzoni & Zuleeg 2011).
Proof demonstrates that psychotropic use in entire population has been increasing tremendously for the past years, however, few studies have investigated that the patterns used to prescribe psychotropic among persons with intellectual disability. Regarding deinstitutionalization, creating warrens of psychotropic use, adverse effects and efforts to minimise its use to individuals with learning disability through the implementation of prescription standards are not clear. Furthermore, with the large as well as representative sample size, it is apparent that there are increased rates of mental illness, challenging behavior and psychotropic medicine among people with intellectual disability.
Research Question
Do challenging behaviors among persons with learning disabilities result from mental impairments?
Are social workers faced with challenges caring for persons with learning disabilities?
Research Objectives
To establish whether or not challenging behaviors among persons with learning disabilities result from mental impairments
To understand some of the challenges that come with caring for persons with learning disabilities
Hypothesis
H0:Challenging behaviors among persons with learning disabilities do not result from mental impairments
H1:Challenging behaviors among persons with learning disabilities do not result from mental impairments
H0:Social workers caring for persons with learning disabilities do not undergo challenges that wear them down
H1:Social workers caring for persons with learning disabilities undergo challenges that wear them down
What is challenging behavior?
An individual’s conduct may be regarded as challenging if it threatens their safety or those around, particularly care or even contributes poor life quality. In addition, such behaviors can influence their capacity to participate in routine activities. Challenging behaviors consist of self-harm, destructiveness and aggression among others. Communication determines the way in which people express their needs.
In the event that communication is problematic, it may extremely discourage individuals leading to challenging behavior. If such behavior contributes to desire results, it may be repeated over and over. Challenging behaviors are common in persons with problems that impact communication and the brain including learning disability, and dementia (Economist Intelligence Unit 2011).
Challenging behavior or behaviors that challenge are culturally anomalous behaviors of frequency or duration that endangers their safety or others. In most cases, an individual must display trends that are a threat to services for a significant timeframe. Seriously challenging behaviors are not transient occurrences. According to the National Institute for Health and Care Excellence (NICE), challenging behavior is a concept that is associated with aggression, stereotype, and agitation or self-harm, withdrawal, and sexual misconduct (NICE 2016).
Additionally, challenging behavior involves persons whose conduct present considerable challenges to services. This comprises of behaviors that are associated with mental health issues. Challenging behaviors are widely used among persons with learning or intellectual disability, in addition to those with autism. Nonetheless, there are other groups that can be regarded to have challenging behaviors such as those with dementia and serious mental issues.
Impact of challenging behavior
Challenging behavior is described as ‘socially unacceptable behavior’, ‘bad behavior’ (Craver 2015). The term also reflects a challenge to those concerned. It indicates that something is not working well, and it needs to be rectified and stopped. Behavior is challenging if it causes harm to another individual, or prevents them from fulfilling certain things in their lives. Challenging behaviors are detrimental to the lives of the affected persons and those around them. Hence, dealing with challenging behaviors requires careful handling in a way that supports the safety and well-being of people and others
Aggression and assault
In a study conducted by 76 social care workers in institutions that provide intellectual disability services, three-quarter of respondents had faced aggression, self-harm, and disruptive behavior. Recent studies of employees working with persons with dementia discovered that roughly three-quarter of workers faced fearful events during their work (Springer et al. 2013). The most common reported cause was physical assault. Among the respondents sampled, a fifth said they had been injured, a quarter experienced fears during interaction, and half of the interviewees stated that they adopted a more personal centered style while others learned to be more vigilant.
This study gives indications of nature and level challenging behavior experienced by staff in care homes for people with dementia. Recent studies of perception of severe behavior and fear of assault showed that the degree of fear was greater when staff was exposed to challenging behavior. Researchers, however, found unclear evidence for the relationship between the quantity of challenging behavior and the level of fear of assault.
Hayes, S. A., & Watson, S. L. 2013. The impact of parenting stress: A meta-analysis of studies comparing the experience of parenting stress in parents of children with and without autism spectrum disorder. Journal of autism and developmental disorders, 43(3), 629-642.
Active duty military is understood as the younger workforce serving the military workforce, where many of the enlisted force comes in between the age of 17 through 24 years old; while seniors of active duty comprises of 27 through 34 years (Wooten, 2015). They are those who are directly or indirectly involved in mobilized military operation including combat. Alcohol abuse has always been common among these active duty military, making ubiquitous practice of heavy drinking as nothing new to the American military system (Larson et al., 2014).
Considered as an accepted custom, drinking is simply considered by military army as a reward for their hard work, and as a commodity that ease their personal tensions since socializing with drinks promotes camaraderie (O’Brien, Oster, & Morden, 2013; Westermeyer & Kimbrel, 2013). There is no denying the fact that heavy drinking is conditioned by the easy availability of alcohol beverages which military personnel received at a reduced rate.
The essay looks into how alcohol consumption has become common among those in active duty military, and how there are risks involved in drinking like physical decline and mental and psychological comorbidities. The essay also provides a conceptual approach towards prevention and treatment of alcohol related issues in military department, by taking up certain structured measures taken up by the government to prevent the cause and spread of alcohol consumption.
Active Duty Military and Alcohol Related Matters in the United States
2.1. Identifying unique PROBLEMS IN Active Duty Military
Earlier, the combat at the Vietnam War caused many military men to become addicted to drugs in 1960 and 1970s, since many were serviced with drugs to make them tolerate the challenges of war environment (O’Brien et al., 2013). Reportedly there was misuse of drugs during this time, and this misuse has been attributed towards the military personnel using drugs for pain relieving and mental trauma issues.
Over the years, prescription of drugs has simply increased because of the availability of more drugs, and because of the wider prescription of medications, followed by intake of alcohol among the military department (O’Brien et al., 2013). This increase in intake of alcohol among military personnel has come to be associated with the recent military combats at Iraq and Afghanistan.
Such increase in the intake of alcohol emanates from many issues associated to their work, like the challenges of war, the stress involved with their work, and experiencing traumatic events that triggers off mental and psychological issues (Robert M. Bray, 2006; Cook, 2007; O’Brien et al., 2013). Many of those engaged in military operations at Iraq and
Afghanistan showed that they have been experiencing stress and strains over long deployments, extreme combat exposure, facing physical injuries, traumatic brain injuries, and post-traumatic stress disorder (PTSD), thereby making them to easily succumb to alcoholic abuse (NIDA, 2011).
Wide availability of prescribing drugs also culminates toward drug abuse. According to the report by NIDA (2011, p. 1), “soldiers screened 3 to 4 months after returning from deployment to Iraq showed that 27 percent met criteria for alcohol abuse and were at increased risk for related harmful behaviors (e.g., drinking and driving, using illicit drugs).” Alcohol usage has also been strongly identified with Post-Traumatic Stress Disorder (PTSD), which comes from the traumatic experiences that military members experienced during the war (Leskin, 2015).
Such suffering culminates towards the victim to fail in becoming good parents and good members of the society, owing to lack of communication and social skills. To quote (NIDA, 2011, p. 1) again, “Mental illness among military personnel is also a major concern. In another study of returning soldiers, clinicians identified 20 percent of active and 42 percent of reserve component soldiers as requiring mental health treatment.
Drug or alcohol use frequently accompanies mental health problems and was involved in 30 percent of the Army’s suicide deaths from 2003 to 2009 and in more than 45 percent of non-fatal suicide attempts from 2005 to 2009.”
Many of the military personnel also consume alcohol simply to experience pleasure. The pursuit of pleasure through alcohol makes them to forego pain, and feel normal or feel euphoric for some time. The reward in term of such sensations allows them to release neurotransmitters called endorphins, thereby experiencing psychological and physiological exhilaration (O’Brien et al., 2013). Such engagement does not lead to any constructive behaviors, but only makes the person to become nonproductive and harmful in nature. Excess of alcohol consumption makes them to suffer from hijacking or from the aberration of normal brain function, thereby making them to become active in their work or when they are deployed.
Excess of alcohol consumption among active duty military men are known to lose their productivity or contract alcohol related diseases that leads to premature death (O’Brien et al., 2013). The difficulty with this situation is that many of them are left untreated, or do not undergo treatment. Thus, the prevention and remedies for alcohol abuse is not only a matter of diagnosis, but it is also about treating the alcohol abusing patients among active duty service members, and also among those in post-deployment stage.
2.2. Comparative Analysis of Active Duty Military with the OVERALL POPULATION of the United States
Although not in similar excess trend with the military personnel, American civilians often resorts to binge drinking occasionally (Cucciare et al., 2015). Access drinking as a problem of the society has simply become a part of American culture, which is slowly degrading the public health and safety system. Even among civilians, alcoholism has always been the problem and the disease, making the National Institute on Alcoholism and Alcohol Abuse (NIAAA) since 1970 to identify ‘alcohol abuse’ as the main national health priorities (Cook, 2007).
Alcoholism related issues such as drunk driving, domestic violence, and other alcohol related abuse is nothing new to the American citizens. Thus, taking social context into perspective, the Americans suffer from innate propensity towards alcoholism, making alcohol consumption a part of their innate culture.
The abuse of alcohol among military and civilians has been acknowledged by the United States military department as having adverse effects on the user’s health and behavior, as well as to their civilian families. It is true that alcohol usage is considered illegal for those who are under the age of 21 in the country, but rampant availability of liquor continue to have negative impact on the functioning of the society as a whole.
This excess of alcohol consumptionhas always been fairly consistent and studies by Westermeyer & Kimbrel (2013) that heavy drinking among military men are always twice as much as military men, and military men also consumes four times higher than military women, while military women consumes twice as more than civilian women. Thus, civilians are as likely to develop alcohol consumption disorders as any military personnel.
Research by Bray et al., (1991) shows that while military people are more likely to consume more alcohol than the civilians, drugs and tobacco are consumed more by the civilians. Drinking within the military group is again higher with the younger military men and women, and even among civilians, intake of alcohol is higher among the younger men and women.
Civilians as well as military efforts to deal with alcohol and drug issues are also directed towards solving the issues of the younger people, so that alcoholic and addiction do not grow on them. Again, many of the military men who suffer from alcohol addiction are higher among unmarried men, which is similar to civilians (Bray et al., 1991). In fact, when demographic comparisons among the unmarried alcoholic men are taken up, addiction and alcohol rate consumption remains the same.
2.3. Treatments and Other Practical Remedies for the issues relevant to the Active Duty Military population
Given the alcohol availability, any military personnel become vulnerable to addiction and are put to risk. To solve the issues of alcohol related issues, several researchers, public health entities, host of government agencies, and laws are working together in the country. Prevention policies in terms of detecting drinking problem at an early stage, and holding specific intervention remains as the best remedy to cure alcoholism.
Treatment and practical remedies in regard to alcohol consumption should initially start with educating the population on how alcohol consumption can lead to risky behavior and how it is harmful to their health (O’Brien et al., 2013). In military department, such policies are enforced during the training process, although effective acknowledgement among the military unit remains inapplicable.
Standard drinking level, like the requirement of not exceeding 14 standard drinks per week for men and 7 drinks per week for women can be imposed or made known to the people, in order to avoid excess consumption (O’Brien et al., 2013). Among military personnel as well as the civilians, environmental strategies prevent alcohol problems remain effective.
These include, raising minimum legal drinking age (21); enforcing the legal minimum purchasing age; increasing taxes on alcoholic drinks; offering no discount to any alcohol beverages; and holding the liquor retailer to be responsible for any issues that comes out of alcoholic drinks (O’Brien et al., 2013). In the words of Cook (2007, p. 1), excess of alcohol consumption can be maneuvered by “both public and private, to reduce excess drinking directly – education, persuasion, counselling, treatment, sanctions of various sorts, [and by ] restricting availability or raising the price – licensing, product and sales regulation, liability rules, taxes, partial or complete bans”.
Owing to many alcohol related cases in military department, the department itself in the United States has also been undertaking comprehensive steps over the past many years to solve these complex issues. Certain legal measures have been taken up by the United States Government to control excess of alcohol consumption among US military personnel from 1980s onward.
This initially started with the Supreme Court of the country declaring in 1988 that the ‘Department of Veterans Affairs’ as not responsible towards paying benefits of alcoholic drinks for the military veterans, since such benefits always results into willful misconduct (O’Brien et al., 2013). In regard to the Department of Defense’s (DoD’s) specifically, they offered series of policies that could help in controlling and preventing the use of alcohol.
The DoD’s effort started in 1970s, when the department passed “The Controlled Substances Act of 1970”, targeting to reduce the usage of drugs at the outset, and later towards smoking and tobacco consumption (Robert M. Bray, 2006). Later, the act also targeted the consumption of alcohol by detection at an early stage and undergoing intervention through law enforced testing (like the urinalysis testing program).
Since legal court disbanded this testing program, DoD later came up with a new measurement that stated that alcohol consumption does not live up to military performance standards (Bray, 2006; Harbertson et al., 2016). Vietnam War and it subsequent result like the prevention of the atrocious war memories that led to high substance abuse among war veterans led to the department to again re-enforced drug and alcohol testing, and emphasizing zero tolerance policies on alcohol and drugs while on duty (Robert M. Bray, 2006; Cook, 2007).
The turn of the millennium saw the DoD and its policies continuing to condemn alcohol abuse (binge or heavy), and other drugs usage, since such abuse brings down the health and the military readiness (active participation) of the military personnel, and since the country needs to maintain high standards of performance and discipline. All such measures are expected deployment military department to decrease their alcohol intake, and perform better as a unit.
3. Finding and Conclusion
It is seen that alcohol abuse remains substantially common among the military personnel that requires stringent efforts on the part of the government (laws and acts), the DoD, medical institutions, and other individual and public efforts to solve and mitigate the issues. Since the Americans involvement in world politics has become popular and regular, military deployment and combat is expected to continue for the American military department.
Contextualizing such issues, the institutions and laws trying to prevent the abuse should use structured approach that will target the entire military populations of the country, and try to mitigate the issue. In this way, the risk to develop alcohol abuse and disorder emanating from such abuse becomes less relevant and less probable in nature. Taking a comprehensive approach to decrease alcohol abuse will allow the fostering of opportunities for military personnel during and after deployment in the field.
It also means that there will be more positive role models for the younger and older citizens to look up to, and also for their own military peer. These efforts to curb alcohol abuse are expected to make military personnel to appreciate and become culturally responsive to military lifestyles and structures.
References
Bray, R. M. (2006). Department of Defense survey of health related behaviors among active duty military personnel: A Component of the Defense Lifestyle Assessment Program. RTI International, (December), 1–307.
Bray, R. M., Marsden, M. E., & Peterson, M. R. (1991). Standardized comparisons of the use of alcohol, drugs, and cigarettes among military personnel and civilians. American Journal of Public Health, 81(7), 865–869. http://doi.org/10.2105/AJPH.2014.301901
Cook, P. J. (2007). Paying the Tab: The Costs and Benefits of Alcohol Control. Princeton: Princeton University Press. Retrieved from https://books.google.co.in/books?id=pMpThh2C6ccC&dq=THE+COST+AND+BENEFITS+OF+ALCOHOL+CONTROL…AUTHOR+PHILLIP+J.+COOK.&source=gbs_navlinks_s
Harbertson, BR, H., EY, A., NL, M., & PT, S. (2016). Pre-deployment Alcohol Misuse Among Shipboard Active-Duty U.S. Military Personnel. American Journal of Preventive Medicine, 51(2), 185–194.
Larson, M. J., Mohr, B. A., Adams, R. S., Wooten, N. R., & Williams, T. V. (2014). Missed Opportunity for Alcohol Problem Prevention Among Army Active Duty Service Members Postdeployment. American Journal of Public Health, 104(8), 1402–1412. http://doi.org/10.2105/AJPH.2014.301901
Leskin, G. (2015). Preventing Substance Abuse in Military Members and Their Families. Prevention Tactics, 9(14), 1–10.
M.A., C., A.G., S., M.A., M., J.C., T., G.M., C., X, H., & B.M., B. (2015). Associations between deployment, military rank, and binge drinking in active duty and Reserve/National Guard US servicewomen. Drug and Alcohol Dependence, 153, 37–42.
NIDA. (2011). Substance Abuse among the Military , Veterans , and their Families. National Institute on Drug Abuse, (April), 1–2.
O’Brien, C. P., Oster, M., & Morden, E. (2013). Substance Use Disorders in the U.S. Armed Forces. Washington DC: National Academy of Sciences.
Westermeyer, J., & Kimbrel, N. A. (2013). Substance Use Disorders Among Military Personnel. In B. A. Moore & J. E. Barnett (Eds.), Military Psychologists’ Desk Reference. New York: OUP USA.
Wooten, N. R. (2015). Military Social Work: Opportunities and Challenges for Social Work Education. Journal of Social Work Education, 51(1), S6–S25. http://doi.org/10.1007/s11121-011-0234-5
Want help to write your Essay or Assignments? Click here