Want help to write your Essay or Assignments? Click here
Sexually Transmitted Infections
This practicum is one of the most fascinating experiences in my clinical practice. Dealing with patients diagnosed with sexually transmitted infections (STIs) is challenging as most of the patient are hesitant to talk openly to a nurse or doctor about their experiences, which makes it challenging during clinical decision making processes (American Congress of Obstetricians and Gynaecologists, 2011).
Mrs. Kate (pseudo name) a 21 year old college student presented to the clinic with complaints of itchiness around her genitalia, sharp burning sensation during sexual intercourse and had noted whitish discharge that had foul smell. From the clinical manifestation, I gathered that the patient is suffering from an infection, which could be either sexually transmitted infections (STIs) or urinary tract infections (UTIs). There is a thin line that separated the two, which indicated the need for further laboratory test.
According to Centre for disease control and prevention (CDC), UTIs and STIs clinical manifestations are non-specific and are a common to problem for females. This highlights the likelihood of misdiagnosis. The common clinical manifestation for the urogenital diseases includes a burning sensation during urination, vaginal discharges and pelvic pain. However, in UTIs infection, vaginal discharge with awful smell is normally absent. The patient with urinary tract infection tends to have fever. A pelvic exam, urine culture and vaginal culture results indicate that the patient had yeast vaginal infection (CDC, 2013).
Want help to write your Essay or Assignments? Click here
One of the challenges experienced during this practicum was during sexual history assessment. Initially, the patient was hesitant to disclose the information because it is a taboo and also she believed that disclosing this information would victimize her. After reinforcing the issue of confidentiality, the patient became relaxed and disclosed the sensitive information.
The sexual history assessment was done using the general guide of the ‘5 Ps.’ This included the number of sex partners, the type of sexual activity, the rates of use of protection, and use of contraceptives. This helped me understand the patient literacy and perspectives about UTI (Schuiling and Likis, 2013).
The patients seemed somewhat distressed when I gave her the diagnosis results. However, she was cooperative all through the care plan. The patient was advised to have regular check up with the gynaecologists. This is because sexually transmitted infections (STIs) have short and long term impacts that can be life threatening. The short term impacts include emotional disturbances due to physical changes.
The long term effects include genital sores, inflammation, infertility issues and pelvic inflammatory reactions. Fortunately, genital yeast infections like other sexually transmitted infections (STIs) is manageable if diagnosed early and proper medication regimen is provided (CDC, 2013).
The patient had tried to manage the itchiness and pain using Tylenol (OTC) and vaginal cream, which yielded little success. The patient was given fluconazole 150 mg and Terconazole 80 mg both orally administered one suppository/day for at least 3 days. The medication ensured that the patient did not get recurrent infection. The patient was encouraged to observe hygiene and practice abstinence during the medication regimen. Other hygiene measures such as mutual monogamy, abstinence and avoid of douching practices.
Want help to write your Essay or Assignments? Click here
This practicum was very enlightening, especially on ways to practice cultural competency. I noticed that sexually transmitted infections (STIs) education focuses in specific information on signs and symptoms which seems to be the worst case scenarios and a taboo to most of the community.
The only down to earth guidance is abstinence and use of condom. If not handled with care, the interaction with the patient could affect patient psychosocial status. I have learnt a lot from this practicum and will use the knowledge to help other patients to identify risk factors and practice preventive measures (Schuiling and Likis, 2013).
References
American Congress of Obstetricians and Gynecologists. (2011). Guideline for adolescent health care (2nd ed.). Retrieved from http://www.acog.org
Centers for Disease Control and Prevention (CDC). (2013). Incidence, prevalence, and cost of sexually transmitted infections in the United States. Retrieved from http://stacks.cdc.gov/view/cdc/13174
Schuiling, K. D., & Likis, F. E. (2013). Women’s gynecologic health (2nd ed.). Burlington, MA: Jones and Bartlett Publishers.
Want help to write your Essay or Assignments? Click here
Want help to write your Essay or Assignments? Click here
Back Pain
Introduction
Back pain is a common and costly disorder in Australia. Hoy et al., (2014) report that about 25% of Australians suffer from back pain and approximately half of them seek medical attention. The direct costs for treatment of this condition in Australia have been estimated to be approximately $ 1 billion with an addition of $ 8 used in indirect costs (Buchbinder et al., 2013).
The condition is also prevalent within the healthcare professionals where nurses have a higher likelihood of developing back pains unlike individuals from other professions. In South Australia alone, back injury accounts for over $2 million in every financial year (Lorig et al., 2013). Surveys of patient self-managing their back pain as well as those managed in primary care have indicated that usual care is not often evidence based hence hindering provision of best outcomes to patients.
Consequently, there has been a growing demand to address the ramifications of back pain through changes in health policies, investments, and service delivery. Healthcare providers, are charged with the responsibility of ensuring that patients receive effective prevention and treatment strategies to curb this menace.
In my visit to John’s home, there are a number of activities that I will conduct to examine John’s condition and the proper intervention that he needs for effective management of his condition. Some of these activities that I will examine include;
Want help to write your Essay or Assignments? Click here
Patient Education
In my initial visit, the first is educating John on chronic back pain. I will highlight clearly that the condition may arise due to an injury or diseases on different body structures such as the muscles, joints, ligaments, or nerves. According to Traeger et al., (2014), the type of pain varies and can be felt as muscle pain, bone pain, or nerve pain. I will also emphasize that it is important for patients to seek medical attention the moment they have back pains and not wait until the disorder worsens to promote effective management of the condition.
At this point, it will be of great significance for me to let John know that he is not the only one suffering from back pain. He should understand that back pain is a massive problem in Australia that sends more people to seek medical attention more than any other condition except common cold (Driscoll et al., 2014).
Nutrition and Weight loss
Normally, patients who are overweight and suffer from back pain, such as John, may not be aware their excess weight aggravates their condition (Brady et al., 2016). It is well known that obese patients are at a greater risk for back pain, muscle strain, and joint pain unlike those that are not overweight. Moreover, obese patients also complain of fatigue and shortness of breath which makes them refrain from exercises worsening their back pain (Heuch et al., 2013).
When patients do not get enough exercise for quite some time, the back’s supporting structures become weak, stiff, and deconditioned which further increases pain (Silisteanu & Covasa, 2015, November). It is for this reasons that I will encourage John to have a weight loss program which may involve gentle low-impact activities such as walking, jogging, or water therapy. I will also advise John to avoid eating foods with high fat content. He should also stick to a rational nutrition plan which involves changes in eating habits as a step toward effective management of his back pain.
During the visit, I will observe John’s posture and position. Reviewing of John’s curvature of the spine, shoulder symmetry, and the iliac crest will also be of great importance. I will conduct a physical examination through palpation of John’s paraspinal muscle to identify any form of tenderness and then initiate proper interventions as per the findings.
Pain Alleviation
For pain reduction, I will encourage John to take timed bed rests and adjust his position to improve flexion of the lumbar region. I will teach him to regulate and adjust the pains that traverse through the respiratory diaphragm. Relaxation can also help in reducing muscle tension that contributes to back pain. John should also adjust his sitting position regularly or even engage in other activities such as reading books, watching a movie or take part in yoga.
I will advise John to request his wife, Donna, to gently massage his back. It has been proven by Kumar, Beaton & Hughes, 2013; Schulz et al., 2014) that massage aids in reduction of muscle spasms, reducing damming, and improve blood circulation.
Want help to write your Essay or Assignments? Click here
Depression
Depression is the most common emotion linked to chronic back pain. Patients with chronic back pain have major depression which is said to be four times greater in such patients than in the general public in Australia. John is not an exception from this statistics since he reports that he is depressed because he can no longer take part in activities such as hiking and cycling that he has always loved.
Research has revealed that depression can trigger back pain (Steffens et al., 2012). It affects the intensity, frequency and the rate of healing of back pain. Consequently, I will advise John to communicate about the depression. Mostly, many patients do not talk to their physicians about their depression, anxiety, or stress (Center, 2012). Individuals that are stressed tend to tense their back muscles which in turn trigger the onset of low back pain or make it even worse.
They believe that the emotions will go away once the initial pain problem is solved. Therefore, John should regularly keep me updated about his feelings so that I may provide desirable care to him. I will also recommend John to interact with other people, for instance, he can occasionally visiting his daughter or son or play with his grandchild to avoid being lonely and stressed up.
The two activities that I will give priority in my subsequent visits are;
Adherence to Medication
Generally, healthcare providers are aware of the considerable increase in rates of opioid prescribing. Opioids have long been used as pain management agents. However, they are associated with adverse reactions such as nausea, vomiting, constipation, respiratory depression, addiction, and even death. The side effects usually limit their use by patients. Therefore, in my first visit and subsequent visits, this is an issue I will be reviewing.
In these visits, I will assess the effectiveness of the prescribed analgesics and inquire from John on whether what he feels after taking the drug. I will then initiate appropriate adjustments according to the patient’s condition for effective pain management. Besides, other pain management therapies such as acupuncture, yoga, chiropractic care, and herbal medicines such as ginger, capsaicin and feverfew can be used (Ferreira et al., 2014).
Want help to write your Essay or Assignments? Click here
ii) Exercise
According to Searle et al., (2015)exercise should be the first treatment choice for a patient with back problems such as John. This is because exercise matches the fact that individuals with chronic back pain should be physically active and involve themselves in their management. Moreover, treatments such as massage, acupuncture, and manipulative therapy are passive hence the patient is not involved in the therapy.
Falla et al., (2014) further highlight that exercise provides other health benefits beyond back pain management, for instance, in terms of bone and cardiovascular health. Therefore, I will encourage John to take part in usually low grade oscillatory exercises such as knees side to side rotation, knee to chest stretches, pelvic tilts, and press ups. I will also help John to come up with an exercise program which I will be supervising to ensure he follows it.
There are several forms of exercise and there is no genuine reason of expecting that one approach would be better than the other (O’Sullivan, 2012; Elden et al, 2013). As a result, I will give John a list of beneficial exercises he can engage in and enquire from him which type he would prefer so that it is included in the exercise program. The best form of exercise for any patient is the one they are enthusiastic about and willing to continue with.
For instance, John says he likes cycling; an activity that has been recorded to have desirable outcomes in patients with back pains. This can be included in his program. I will advise John not to take part in heavy physical activities, circular motions, and sways which often worsen the condition. I will encourage John to switch activities while sitting, lying or walking for a long time.
Want help to write your Essay or Assignments? Click here
Conclusion
Back pain is a common health problem in Australia (Cramer et al., 2013). However, its prevalence can be reduced significantly if patients and clinicians work together. Patients, for instance, should seek early medical attention and adhere to the prescribed medications and the recommended activities. On the other hand, physicians should keep a close surveillance on these patients and ensure that desirable patient outcomes are realized.
References
Brady, S. R., Hussain, S., Brown, W. J., Heritier, S., Billah, B., Wang, Y., & Cicuttini, F. M. (2016). Relationships between weight, physical activity and back pain in young adult women. Osteoarthritis and Cartilage, 24, S10-S11.
Buchbinder, R., Blyth, F. M., March, L. M., Brooks, P., Woolf, A. D., & Hoy, D. G. (2013). Placing the global burden of low back pain in context. Best Practice & Research Clinical Rheumatology, 27(5), 575-589.
Center, C., Relief, P., Covington, L. A., & Parr, A. T. (2012). Caudal epidural injections in the management of chronic low back pain: a systematic appraisal of the literature. Pain Physician, 15, E159-E198.
Depression Goesling, J., Clauw, D. J., & Hassett, A. L. (2013). Pain and depression: an integrative review of neurobiological and psychological factors. Current psychiatry reports, 15(12), 1-8.
Driscoll, T., Jacklyn, G., Orchard, J., Passmore, E., Vos, T., Freedman, G., & Punnett, L. (2014). The global burden of occupationally related low back pain: estimates from the Global Burden of Disease 2010 study. Annals of the rheumatic diseases, annrheumdis-2013.
Elden, H., Gutke, A., Kjellby-Wendt, G., Fagevik Olsén, M., Stankovic, N., & Östgaard, H. C. (2013). Back pain in relation to pregnancy: A longitudinal 10-year follow-up of 369 women diagnosed with pelvic girdle pain during pregnancy. In Advances in multidisciplinary research for better spinal/pelvic care. The 8th Interdiciplinary World Congress on Low Back & Pelvic Pain, Oct, 2013. Dubai.
Falla, D., Gizzi, L., Tschapek, M., Erlenwein, J., & Petzke, F. (2014). Reduced task-induced variations in the distribution of activity across back muscle regions in individuals with low back pain. PAIN®, 155(5), 944-953.
Ferreira, P. H., Ferreira, M. L., Maher, C. G., Refshauge, K. M., Latimer, J., & Adams, R. D. (2013). The therapeutic alliance between clinicians and patients predicts outcome in chronic low back pain. Physical therapy, 93(4), 470-478.
Heuch, I., Heuch, I., Hagen, K., & Zwart, J. A. (2013). Body mass index as a risk factor for developing chronic low back pain: a follow-up in the Nord-Trøndelag Health Study. Spine, 38(2), 133-139.
Hoy, D., March, L., Brooks, P., Blyth, F., Woolf, A., Bain, C., & Murray, C. (2014). The global burden of low back pain: estimates from the Global Burden of Disease 2010 study. Annals of the rheumatic diseases, annrheumdis-2013.
Kumar, S., Beaton, K., & Hughes, T. (2013). The effectiveness of massage therapy for the treatment of nonspecific low back pain: a systematic review of systematic reviews. Int J Gen Med, 6, 733-741.
O’Sullivan, P. (2012). It’s time for change with the management of non-specific chronic low back pain. British journal of sports medicine, 46(4), 224-227.
Schulz, C., Leininger, B., Evans, R., Vavrek, D., Peterson, D., Haas, M., & Bronfort, G. (2014). Spinal manipulation and exercise for low back pain in adolescents: study protocol for a randomized controlled trial. Chiropractic & manual therapies, 22(1), 1.
Silisteanu, S. C., & Covasa, M. (2015, November). Reduction of body weight through nutrition intervention reduces chronic low back pain. In E-Health and Bioengineering Conference (EHB), 2015 (pp. 1-3). IEEE.
Steffens, D., Ferreira, M. L., Maher, C. G., Latimer, J., Koes, B. W., Blyth, F. M., & Ferreira, P. H. (2012). Triggers for an episode of sudden onset low back pain: study protocol. BMC musculoskeletal disorders, 13(1), 7.
Traeger, A. C., Moseley, G. L., Hübscher, M., Lee, H., Skinner, I. W., Nicholas, M. K., & Hush, J. M. (2014). Pain education to prevent chronic low back pain: a study protocol for a randomised controlled trial. BMJ open,4(6), e005505.
Want help to write your Essay or Assignments? Click here
Lack of Proper Education on Patient with Type 2 Diabetes
Want help to write your Essay or Assignments? Click here
Lack of proper education on patient with type 2 diabetes
Locating the Best Evidence
Often, type 2 diabetes patients lack proper education mainly because of the different barriers that they face as well as the receiving education that lacks a proper algorithm. Therefore, there is a great need for these measures to be acted upon so that the patients can realize more positive outcomes. Mshunqane, Stewart and Rothberg (2012) indicated that diabetes type 2 is associated with numerous complications, many of which can cause death if not managed appropriately.
In addition to this, at the worldwide level, the disease is acknowledge as a main challenge that nags the policymakers each day. There is presently some staggering statistics of the increasing prevalence as well as the linked economic and health impact.
Further, the World Economic Forum, World Health Organization, as well as the United Nations recognize the challenge. All these bodies suggest for collective dedication to improve the life quality of the patients as well as prevent the disease. They are clear that the challenge is universal, urgent, and critical. There is also the acknowledgment that the disease is serious for two main reasons (Stults-Kolehmainen & Sinha, 2014).
First is the health impacts linked to it which are more critical including increased likelihood for lower limb amputations, blindness, heart attacks, kidney failure, as well as stroke. Second, there are indirect and direct costs which are a major drain on the healthcare budgets as well as productivity.
The issue is very urgent considering that its prevalence is rising. Moreover, managing the complications associated with the disease is very costly, same as incorporating appropriate measures to ensure that the patients lead a high quality and independent life. The mentioned bodies also agree that proper education is one of the strategies through which the disease can be prevented and managed efficiently.
However, there are a number of barriers that prevent this and the education algorithm normally used is inappropriate. Therefore, this systematic review will aim at finding information suggesting the appropriate algorithm as well as the common barriers as well as how they can be addressed.
Want help to write your Essay or Assignments? Click here
Methods
Search strategy
Peer-reviewed academic journals will be sought from different databases, and these will be used to conduct the systematic review (Lee et al., 2013). The intention will be creating a proper algorithm on diabetes type 2 education, as well as identify some of the barriers to proper education and how they can be addressed. The databases to be used for the systematic review are CENTRAL, Social Science Citation Index, Science Citation Index, PSYCLinfo, Medline, ERIC, and CINAHL.
The references to the articles that were selected were also evaluated for leads. Reading the reviews was necessary as it helped identify if the article was appropriate. In relation to the inclusion criteria, there was selection of articles that were not older than five years. Particularly, there was selection of those discussing the barriers to proper diabetes type 2 education and their solutions, and those discussing proper education standards (Kapoor & Kleinbart, 2012).
Critically Analyzing the Evidence and Synthesis
Proper education algorithm
Type 2 diabetes education preventive measures will be informed to all the people through local barazas. This would ensure that all people engage in appropriate lifestyles to prevent the disease. Cultural competent educators, and those with proper listening and communication skills will be used to offer the education so that no one can be left behind (Garber, Gross & Slonim, 2010).
It will be necessary to educate the patients on all aspects of the disease including the causes, risk factors, predisposing factors, preventive strategies, available treatments, and management. In addition, awareness on how a patient can ensure self-care should be offered, same as the complications and the direct and indirect costs that a family can suffer because of the disease.
Moreover, the educator should go into details when elaborating on the preventive measures including the diet and physical activity. The more the patients and all people know about the disease and how it is connected to other chronic conditions, the more efficiently they can engage in self-care (Green, 2014).
Barriers and addressing them for patients to be able to receive the recommended type 2 diabetes education, they should really be concerned about their healthcare and ready to access or seek quality medical education. However, because of the ignorance some patient have, they prefer using over-the-counter medications or seeking traditional medicine men. They never seek the quality healthcare services because of their ignorance and low socioeconomic backgrounds.
Therefore, even the use of preventive services among these patients is very minimal. To address this, the local authorities will be given a chance to mobilize people from their living areas, so that education can start at the grassroots level before even being offered at the healthcare institution (Zoepke & Green, 2012).
In addition, there are many elderly people suffering from type 2 diabetes and with hearing, memory, and vision challenges. These will be offered the education in the presence of caregivers who can assist them around (Chijioke, Adamu &Makusidi, 2010).
Feasibility, Benefits, and Risks
Feasibility
The project of delivering proper education to the type 2 diabetes, patients is feasible, especially if the most appropriate education is being delivered, with a consideration of the personal factors, and if the barriers that might hinder the education have been considered and measures to address these put in place. Healthcare providers would only need to offer patients attending the institution for medical care services the pamphlets containing all the necessary information.
However, when dealing with type 2 diabetes patients, it would be necessary to find out first what they already know and later creating awareness while dispelling the misconceptions. This would be relatively cheap. It would also be necessary to explore other factors that affect individual patients so that advice can be offered (Rosenstock & Owens, 2008).
Barriers
After proper education is offered and the barriers to it addressed, some patients might still lack the funds to purchase even the affordable local foods. Considering that some patients might be elderly, there might be issues such as improper vision, hearing loss, and memory loss, which might influence practice of the education.
Benefits
Ensuring that the patients are receiving proper education and implementing it is essential in that it can go a long way in reducing the high prevalence of the disease, preventing complications, reducing the high costs needed to treat and manage the condition, as well as the losses related to loss of productivity and need for a higher quality of life (Ruffin, 2016).
Risks
Some of the anticipated risks include limited resources to ensure that adequate and proper education on type 2 diabetes is being delivered to the patients (Valencia &Florez, 2014). In addition, there might be absence of cultural competence professionals to deal with patients from different backgrounds. In addition, tracking the patients at their homes to ensure that they are implementing the proper education appropriately can be difficult and costly.
Garber, J. S., Gross, M., & Slonim, A. D. (2010). Avoiding common nursing errors. Philadelphia: Wolters Kluwer Health/Lippincott Williams & Wilkins.
Green, B. (June 06, 2014). Diabetes and diabetic foot ulcers : an often hidden problem : review. Sa Pharmacist’s Assistant, 14, 3, 23-26.
Kapoor, B., & Kleinbart, M. (2012). Building an Integrated Patient Information System for a Healthcare Network. Journal of Cases on Information Technology (jcit), 14, 2, 27-41.
Mshunqane, N., Stewart, A. V., & Rothberg, A. D. (January 01, 2012). Type 2 diabetes management : patient knowledge and health care team perceptions, South Africa : original research. African Primary Health Care and Family Medicine, 4, 1, 1-7.
Rosenstock, J., & Owens, D. (January 01, 2008). Treatment of Type 2 Using Insulin: When to Introduce?.
Ruffin, T. R. (January 01, 2016). Health Information Technology and Change.
Stults-Kolehmainen, M. A., & Sinha, R. (January 01, 2014). The Effects of Stress on Physical Activity and Exercise. Sports Medicine, 44, 1, 81-121.
Valencia, W. M., &Florez, H. (January 01, 2014). Pharmacological treatment of diabetes in older people. Diabetes, Obesity & Metabolism, 16, 12, 1192-203.
Zoepke, A., & Green, B. (January 01, 2012). Diabetes and diabetic foot ulcers : an often hidden problem : general review. Wound Healing Southern Africa, 5, 1, 19-22.
Want help to write your Essay or Assignments? Click here
Weight Management for Overweight/Obese Children: Parents Take Charge (PTC)
Want help to write your Essay or Assignments? Click here
Weight Management for Overweight/Obese Children: Parents Take Charge (PTC)
Abstract
This proposal is designed to halt the increasing rate of childhood obesity. Modifications in nutrition, behavior and physical activity are well documented to produce successful outcomes for obesity with the main change agent being the individual. Due to the complexities of childhood obesity, an intervention that includes proven elements that prevent obesity and addresses the special factors that affect children is needed.
Parents Take Charge (PTC) is a multi-component family-based childhood obesity intervention that includes modification in nutrition, behavior and physical activity, but focuses on the parent(s) being the primary change agent for the child, age 10-13 years. Addressed in this evidenced-based proposal are the assessment of need, an analysis of best evidence, design aspects, implementation, evaluation, integration and maintenance of the practice change in a primary care setting.
The focus of the intervention is to teach healthy lifestyle behaviors to the child through parental involvement instead of focusing on weight reduction as the primary outcome.
Weight Management For Overweight/Obese Children: Parents Take Charge (PTC)
Quality care can be defined as appropriately identifying, evaluating, diagnosing and treating patients. The term quality in healthcare is correlated to professional knowledge and desired health outcomes (Institute of Medicine, 2012). It is also defined as being closely associated with patient safety (Mitchell, 2008). Clinical excellence is the goal of providing quality care. The process for achieving clinical excellence includes patient-centered care.
The patient is the focus and includes their concerns regarding their illness, values, beliefs and support network. Making the patient an active participant in their health care results in informed decision-making by the patient. Autonomy, nonmalfeasance, beneficence, justice and fidelity are ethical principles that are addressed as definitions of providing quality care and achieving excellence in primary care.
America Nurses Association, American League of Nursing, and Center for Applied and Professional Ethics are organizations that set guidelines for excellence (Stanley, 2011). Quality and excellence in a clinical site is achieved through appropriate, comprehensive and timely care.
Examples of methods of providing clinical excellence include providing evidence-based treatment, the timely manner in which patients are seen from when they sign in, the offer of generics versus brand-name medications, patient education, open dialogue with patients and referrals to specialist as needed. Ethical considerations taken in account are the patient’s autonomy. The patient is provided information for full understanding of their illness, evaluation, treatment and alternative treatments so that the capability for informed decision-making is established.
Guidelines for the prevention, identification, assessment and management of overweight and obesity in adults and children include how to assess whether people are overweight or obese; what should be done to help people lose weight; how to care for people who are at risk due to their weight and how to help people improve their diets and increase their physical activity (The National Institute for Health and Clinical Excellence NHS, 2012).
The intention of this paper is to present an evidence-based project (EBP) proposal for childhood obesity. Included in this paper is assessing the need for change in practice, appropriate theoretical models and frameworks, statement of problem, intervention, goals, systematic review of current research and design. Assessing the need for change in practice consists of identifying stakeholders, collecting internal data about current practice, comparing external data with internal data, identifying the problem and linking the problem with interventions and outcomes (Larrabee, 2012).
Step 1: Assessing the Need for Change in Practice
Stakeholders
The first step for the model of evidenced-base change is assessing the need for change in practice. To facilitate this, identification of stakeholders is needed. The target population is children, age 10-13 years and their families. Final decisions to change behaviors lies with the children, but parents have great influences over the young child’s meals, snacks and physical activities.
Participating parents therefore, will be the change agent, adding them to the list of stakeholders. Parents make informed decisions regarding the health of their children with the help of a primary healthcare provider (Burns, Dunn, Brady, Starr, & Blosser, 2013). Primary healthcare providers or nurse practitioners (NPs) are stakeholders that will assist in facilitating and implementing change.
Barriers to Change
Barriers for children’s outcomes include their maturity level; ability to understand or commit to the program and their parents, if they are reluctant to participate. The primary barrier to change is participation of the parents. Physical activity and dietary behaviors will need modification in and out of the home. Without the participation of the parents the goal for long lasting results will not occur.
Barriers for the parents include health literacy level; language, if the primary language is not English and attitudes towards modifying foods and physical activity. Another barrier is the participant’s adherences to the nutritional guidelines provided because diet plans do not include the cultural foods that the family consumes.
Want help to write your Essay or Assignments? Click here
Facilitators to Change
Facilitators to change include support from their primary care provider or NP that the participants know and trust, educational classes that will be designed to meet their family’s cultural and specific needs and physical activities that can be done as a family that includes utilizing the workout facilities and pool in the local gym.
Internal Data
Internal data (date retrieved within Porterville Valley PromptCare Medical Center) provides overweight/obesity information that is defined by height, weight, body mass index (BMI), frequency of physical activity and anthropometric measurements of children in rural Tulare County, California.
External Data
External data (data retrieved outside of Porterville Valley PromptCare Medical Center) include the following (Ogden, Carroll, Kit & Flegal, 2012; California Center for Research on Women & Families, 2011):
a). Approximately 31.8 percent of children and adolescents aged 2—19 years are obese in the United States
b). Approximately 1 in 3 (33.2 percent) of children and adolescents age 6 to 19 years are considered to be overweight or obese in the United States
c). An estimated 30.5% of children and adolescents aged 10-17 years are presently overweight or obese in California
d). The total percentage of overweight and obesity from 1999 to 2009 rose from 34.0% to 37.6% for 9-11 year olds in California
e). For teens ages 12-17 years in California, African American youth had the highest percentage of overweight/obesity (39.9%), followed by Latinos (29.4%), Asian/other (18.0%) and white youth (12.0%)
Internal data presents an estimated 30% of the children seen in Porterville Valley PromptCare Medical Center are overweight or obese. When comparing Internal data and External data a change in practice is needed to prevent the incidence of childhood obesity from continuing to grow at an alarming rate.
Want help to write your Essay or Assignments? Click here
Theoretical Model and Framework
Since this EBP proposal involves changes in physical activity and dietary behaviors understanding the effects of behavioral and social aspect of the child is necessary. With this in mind, the Transtheoretical Model will be discussed as an integral element in the design of PTC, an overweight/obese child intervention proposal.
Transtheoretical Model (TM)
The TM integrates clinical psychology and concepts to support a framework to understand the behavior and motivate behavioral change. The concepts of TM are decisional balance, processes of change, self-efficacy and temptation. The five stages of the transtheoretical model are the following: precontemplation (not intending to change), contemplation (considering a change), planning or preparation (actively planning change), action (actively engaging in a new behavior) and maintenance (taking steps to sustain change and resist temptation to relapse) (Kadowki, 2012).
Decisional balance occurs in each stage and involves the weighing of advantages and disadvantages towards changing behavior. The processes of change are the steps that facilitate understanding and behavioral change. Self-efficacy is essential and will vary depending on the TM stage. Temptation to revert back to previous stages will exist throughout the model. Support from the individual’s social network will provide the encouragement to continue within the program’s parameters.
Problem
A correlation between obesity and chronic diseases such as cardiovascular disease, diabetes mellitus and hypertension has been documented. Life expectancy for those who are obese is lower than those that maintain a normal Body Mass Index (BMI) (Centers for Disease Control and Prevention, 2011). Earlier death rates in adulthood have been linked to excess weight in the younger ages (American Heart Association, 2013).
The prevalence of obesity has increased three-fold over the past few decades and is reported as a public health problem within the United States (Singh & Kogan, 2010). The cost of health care for obesity-related diseases (diabetes mellitus, hypertension, cardiovascular disease, etc) has skyrocketed and is predicted to continue to grow.
In the year 2000 an estimated $117 billion and $61 billion was spent both directly (medical costs) and indirectly (lost work time, disability, premature death and subsequent loss of income, etc) on overweight and obese individuals in the United States (Ward Smith, 2010). Chronic diseases linked to obesity were once seen mainly in adults, but are now becoming more and more prevalent in children.
The National Center for Chronic Disease Prevention and Health Promotion (NCCDPHP), Division of Adolescent and School Health (2010) reported “the prevalence of obesity among children aged 6 to 11 years increased from 6.5% in 1980 to 19.6% in 2008…and among adolescents aged 12 to 19 years increased from 5.0% to 18.1%” (NCCDPHP, Division of Adolescent and School Health, 2010). Health concerns for obese children are a reality that must be addressed since the effects of early obesity will impact their health for the rest of their lives.
Want help to write your Essay or Assignments? Click here
Problem Statement
The problem addressed in this EBP proposal is the growing rate of childhood obesity and the negative effects on the child, parents, family and community.
Possible Interventions
Intervention of childhood obesity includes early identification and participating in health promotion activities such as eating healthier and becoming more physically active, as early as possible, to reduce the likelihood of chronic diseases and increase the health in those at risk. Wojcicki and Heyman (2010) stated “studies have shown that early interventions can potentially prevent the development of obesity in school-age children, along with associated health conditions” (Wojcicki & Heyman, 2010, p. 1457).
Interventions of childhood obesity include promoting a balanced diet and increased frequency of physical activity. But, with the complexity behind childhood obesity, it requires other interventions as well. Vos, Wit, Pikl, Kruff and Houdijk (2011) stated their family-based cognitive behavioral multidisciplinary lifestyle treatment “aims to establish long-term weight reduction and stabilization, reduction of obesity related health consequences and improvement of self-image by change of lifestyle and learning cognitive behavioral techniques” (Vos et al., 2011).
Education and physical activity should be provided to the whole family in order to ensure successful lifestyle change to occur for the child. It is hoped that by encouraging whole family participation that a lasting positive outcome would result.
Pender, Murdaugh and Parsons (2011) stated “the significant role the family plays in the development of both health-promotion and health-damaging behaviors, beginning at a very early age is well documented” (p. 243). Golley, Magarey, Baur, Steinbeck and Daniels (2007) stated “parenting-skills training combined with promoting a health family lifestyle may be an effective approach to weigh management in prepurbertal children, particularly boys” (p. 517).
Critical Outcome Indicators
Outcome indicators aim to achieve results that matter to the patient (Larrabee, 2012). Critical outcome indicators include improved BMI, improved laboratory measurements, improved health behavior, improved dietary patterns and increased frequency of physical activity.
Goals and Purpose
The health goal is to improve outcomes of obese children living in rural Tulare County, California. Quality goals are to improve access to diagnostics, early treatment and continuity of care with the use of evidence-based practices that include family participation. Quality measures include the participant’s understanding of the nature of obesity, treatment, the negative impact of obesity on lifestyle and overall health. These aspects will be measured through documentation of BMI status, weight classification, percent of physical activity and nutritional counseling.
Purpose Statement
The purpose of the EBP proposal is to promote health and well being in overweight/obese children and their whole family through participation in a nine-week multi-component, family-based community intervention program.
Want help to write your Essay or Assignments? Click here
Want help to write your Essay or Assignments? Click here
Designing a Practice Change
Introduction
Trends have indicated an increase in prevalence in diabetes with 42% of the patients with diabetes aged over 65 years (Chen et al., 2012). Projections have been conducted and proved that this ratio will increase to over 60% by 2050. This increase in diabetes prevalence has also impacted related health care costs.
For instance, the average acute hospital cost for managing diabetic patient with a diabetic foot was estimated to be $9,900 in the USA (Dabelea et al, 2014). According to Wong et al, this rise in the prevalence of diabetes has made it imperious to offer training and practice care for clinicians to manage diabetes (Wong et al., 2015).
This paper is going to focus on the design of Evidence Based Practice training program for practice change that will be aimed at training healthcare practitioners on diabetes and improving the outcomes of patients with diabetes.
Timeline
The training module will involve one basic 50-minute presentation which will be conducted by a well-trained diabetes educator and a physician. The presentation will be conducted on Monday, Wednesday and from 0800hrs to 0850hrs for a period of two months. The presentation will be divided into two parts.
The first part will concentrate on enlightening the trainees on diabetes for practice change, that is, the causes, risk factors, onset, types, signs and symptoms, treatment, and management of this disease. This part will also highlight the complications associated with diabetes. The second part of the presentation will concentrate more on patient education which is an integral component of comprehensive patient care.
Several long term care facilities will be contacted as potential recruitment sites. Comprehensive training modules and assessment measures will also be developed to aid in the evaluation of immediate and long term impact of the training project.
Want help to write your Essay or Assignments? Click here
Key Personnel
To achieve the educational needs of the clinicians the program will focus on training licensed practical nurses (LPNs), registered nurses (RNs), and physical therapists. The module will conduct a follow-up of learning outcomes in one group (RNs). The training will be designed for a small group of between 20-30 trainees in each session. This will ensure that close interaction is maintained between the participants and the instructors, with time set aside for participant comments and questions.
Want help to write your Essay or Assignments? Click here
Supplies Needed
Some of the material that will be required include; PowerPoint presentation, videos, and handouts.
PowerPoint Presentation: Will consist of 40 slides. These slides will entail a brief overview of diabetes, and the associated complications such as foot problems, risk of amputation, blurred vision, and kidney problems. It will also offer information on appropriate history taking, keeping of records, conducting physical examination, and appropriate specialist referral.
Video: This will demonstrate the proper techniques of carrying out patient examination such as conducting a monofilament examination with the aid of a tuning fork.
Handout: Will be issued to the participants for daily patient explaining and for explaining how to conduct physical examination on a patient with diabetes.
An official website that will contain all that will have been taught during this period.
Cost
For successful completion of this module, funds will be used in paying two diabetes instructors, paying the IT technicians who will compile the PowerPoint presentation, the video, creation of website and typing of the handout. Funds will also be used in buying enough training materials such as tuning forks for the monofilament examination and glucometers. All this will be allocated a total of $ 2,000.
How do these items tie up to project goals?
These items will help in achieving the set goal of 10-15% increase in diabetes practice change two month post training. Such training promotes clinical judgment and advance patient care quality. The clinicians will understand how to acquire, interpret, and incorporate the best available research evidence with clinical observations and patient data which are important aspects in clinical practice (Wong et al., 2015).
Dabelea, D., Mayer-Davis, E. J., Saydah, S., Imperatore, G., Linder, B., Divers, J., … & Liese, A. D. (2014). Prevalence of type 1 and type 2 diabetes among children and adolescents from 2001 to 2009. Jama, 311(17), 1778-1786.
Wong, C. K. H., Wong, W. C. W., Wan, Y. F., Chan, A. K. C., Chan, F. W. K., & Lam, C. L. K. (2015). Effect of a Structured Diabetes Education Programme in Primary Care on Hospitalizations and Emergency Department visits among people with type 2 diabetes mellitus: results from the Patient Empowerment Programme. Diabetic Medicine.
Wong, C. K., Wong, W. C., Wan, Y. F., Chan, A. K., Chan, F. W., & Lam, C. L. (2015). Patient Empowerment Programme (PEP) and Risk of Microvascular Diseases Among Patients With Type 2 Diabetes in Primary Care: A Population-Based Propensity-Matched Cohort Study. Diabetes care, 38(8), e116-e117
Want help to write your Essay or Assignments? Click here
Want help to write your Essay or Assignments? Click here
Feasibility, Benefits, and Risks
Feasibility of the implementation of change in practice
Undeniably, several studies have reported on the dramatic increase of Diabetes type 2, especially among people below 30 years. This dramatic increase and complications associated with the disease are important public health issues that feasibility must be addressed amicably. Recent surveys have recommended that the application of education strategies facilitates changes in lifestyle among patients diagnosed with diabetes Type 2.
This is specifically in subjects identified as high risk of developing diabetes type 2. Research indicates that integration of the proposed practice in the clinical setting will reduce approximately 60% risk of developing diabetes Type 2 within 3 years of intervention. Secondly, the effects of these interventions are long- term (Inzucchi, et al., 2012).
Want help to write your Essay or Assignments? Click here
Potential barriers for the implementation
One of the major barriers for the implementation of the practice is inadequate resources. This will make it difficult for the healthcare providers to balance between their workloads and the demand of practicing proposed intervention- integrative patient education. Other potential barriers are organizational cultural and policy barriers that could lead to staff resistance.
Due to the low level of research in the clinical setting, most of the healthcare providers would be sceptical regarding the evidence based research. Therefore, prior to the onset of the research, the healthcare providers will be trained to ensure they understand the concept and project outcomes (Inzucchi, et al., 2015).
Main Risks of the integration of the practice
The main risk involved in integration of the practice into the clinical setting is the concern that too much content about diabetes type 2 could result in confusion and reduce its utility. Additionally, communication barriers could reduce the opportunity for the patient-physician interaction, which would make it difficult to realize the project’s objectives (Steinsbekk, et al., 2012).
Want help to write your Essay or Assignments? Click here
Benefits for integration of the practice into the clinical setting
Integrative patient education is beneficial as it will increase the patient’s ability of understanding the disease pathophysiology, and in establishment of the relevant coping strategies. This is because it will facilitate the process of diagnosis and treatment alternatives, as well as the consequences of various patient activities. Additionally, it will help the patient to make appropriate decision, thereby reducing the readmission rates, length of hospitalization and slows the disease progression (Kayshap et al., 2013).
The intervention justifies the time as well as cost toward the improvement of the feasibility of clinical outcomes.
The proposed study is an expensive study as it involves a lot or resources such as educating material, employment of additional nurse assistants and time. However, the outcome of the ontervention justifies these costs as it increases patients satisfaction, improve the patient compliance to the regulatory standards and improve the efficiency of care. Lastly, better informed patients are more alert and attentive, which minimizes the risk of malpractice.
Ethical concerns
The researcher will seek permission from ethical review board committee at the institution. The work will require to be approved by the IRB as it involves interaction with human beings. This is to ensure that the study is safe and does not pose potential dangers to the participants. Each of the participants will be required to fill in a consent form.
Inzucchi, S. E., Bergenstal, R. M., Buse, J. B., Diamant, M., Ferrannini, E., Nauck, M., … & Matthews, D. R. (2015). Management of hyperglycemia in type 2 diabetes, 2015: a patient-centered approach: update to a position statement of the American Diabetes Association and the European Association for the Study of Diabetes. Diabetes Care, 38(1), 140-149.
Steinsbekk, A., Rygg, L., Lisulo, M., Rise, M. B., & Fretheim, A. (2012). Group based diabetes self-management education compared to routine treatment for people with type 2 diabetes mellitus. A systematic review with meta-analysis. BMC health services research, 12(1), 213.
Want help to write your Essay or Assignments? Click here
Want help to write your Essay or Assignments? Click here
Dementia PICO Analysis Method
Part I: PICO analysis of research topic
Step 1: Frame clinical question using PICO method
P: the patients include people with dementia and psychosis
I: the anticipated intervention is to utilize typical antipsychotic drugs
C: the current standard or comparison group is atypical antipsychotics
O: the desired outcome is to have less mortality rates for elderly people with dementia and psychosis
The PICO question basically stands for patient, intervention, comparison and outcome (Elkins, 2014).
Part II: Search strategy
The PICO question is as follows: In elderly patients who have dementia and psychosis (P), does treatment with typical antipsychotics (I) or atypical antipsychotics (C) result in less mortality (O).
Step 1: Resources utilized to find articles
A number of scholarly articles relating to the identified issue are identified. The resources that were used in finding the articles that relate to the topic include the following: handbooks, electronic databases research, encyclopaedias, relevant books, and reputable journals.
Step 2: Search terms and criteria
With regard to search terms and criteria that were utilized, the search terms include the following: dementia, mortality, psychosis, atypical antipsychotics, and typical psychotics. The inclusion criteria was as follows: scholarly peer-reviewed journal articles only, articles not older than 5 years, articles that are published in the English language, articles that focus on dementia and psychosis among the elderly population, and article that reports on primary research.
Step 3: Boolean search strings
With regard to the exclusion criteria, the articles that would be excluded are as follows: articles that are older than 5 years, articles not published in English, and articles that do not focus on the elderly patients with dementia. Using different Boolean search strings, keywords would be combined with operators like OR, NOT as well as AND in order to generate additional results that are relevant. For this research, the Boolean search strings that would be utilized include the following: atypical antipsychotics and psychosis, atypical antipsychotics and dementia, typical antipsychotics and dementia, typical antipsychotics and psychosis. Therefore, the search results would be limited only to the two keywords.
Want help to write your Essay or Assignments? Click here
Part III: Analysis of literature
Step 1: Summary of five articles
The following 5 articles in the table below were selected from the research effort.
Table 1: Summary of analyzed articles
Citation
Conceptual framework / theory
Main finding
Research Method
Strengths of study
Weaknesses of study
Level of evidence
Ballard, C., Creese, B., Corbett, A., & Aarsland, D. (2011). Atypical antipsychotics for the treatment of behavioural and psychological symptoms in dementia, with a particular focus on longer term outcomes and mortality. Expert Opinion on Drug Safety, 10(1): 35-43
Not specified
Atypical antipsychotics medications provide modest benefits up to twelve weeks /short term treatment of psychosis and dementia. Nonetheless, these benefits should be balanced against the risk of major adverse events such as increased death. With longer term prescribing, there are clear benefits, but the risk of death also increase.
Review of existing studies. The authors provide a summary of the evidence that pertain to safety and efficacy from short-term randomized controlled trials, as well as main findings from case register studies
Study is thorough. Presents both benefits and shortcomings of atypical antipsychotic drugs. The review provides an up-to-date and balanced overview of the safety concerns and effectiveness that relate to atypical antipsychotics in elderly patients with dementia, giving a full overview of mortality risk
The study only focuses on atypical antipsychotic drugs and does not also look into the safety concerns and efficacy of typical antipsychotics.
High level
Haddad, P. M., & Sharma, S. G. (2012). Adverse effects of atypical antipsychotics: Differential risk and clinical implications. CNS Drugs, 21(11): 911-936
Not specified
Broad statements that compare the comparative risk of specific adverse effects between conventional and atypical antipsychotics are mainly insignificant. Instead, comparisons need to be made between particular typical and particular atypical antipsychotic drugs.
The authors reviewed various studies including post marketing, surveillance studies, and observational studies and randomized controlled trials.
The study is comprehensive, thorough and up-to-date
A small number of studies were reviewed
High level
Piersanti, M., Capannolo, M., Turchetti, M., Serroni, N., De Berardis, D., Evangelista, P., Costantini, P., Orsini, A., Rossi, A., & Maggio, R. (2014). Increase in mortality rate in patients with dementia treated with atypical antipsychotics: A cohort study in outpatients in Central Italy. Riv Psichiatr, 49(1): 34-40
Not specified
Using atypical antipsychotics to treat dementia amongst older adults is linked to a higher rate of mortality.
A cohort study was conducted that comprised 696 elderly patients with Alzheimer
The study recommends new approaches for managing dementia to replace the use of atypical antipsychotic drugs which have potential risks of mortality
A small sample size was used and the study was carried out within a single hospital. This affects the generalizability of the findings
Medium level
Rochon, P. A., Gruneir, A., Gill, S. S., Wu, W., Fischer, H. D., Bronskill, S. E., & … Gurwitz, J. H. (2013). Older Men with Dementia Are at Greater Risk than Women of Serious Events After Initiating Antipsychotic Therapy. Journal Of The American Geriatrics Society, 61(1), 55-61. doi:10.1111/jgs.12061
Not specified
Shortly after initiating oral atypical antipsychotic drug, the likelihood of developing a major event in elderly people with dementia was high.
This was a population-based, retrospective cohort study.
A large sample size was used that comprised 21,526 elderly men and women with dementia
The study had more women that. Women were 13,760 while the number of men was 7,766.
High level
Schneider, L. S., Dagerman, K. S., & Insel, P. (2012). Risk of death with atypical antipsychotic drug treatment for dementia – Meta-analysis of randomized placebo-controlled trials, JAMA, Journal of the American Medical Association, 294(15): 1934-1943
Atypical antipsychotic medicines might be linked to a slight increased likelihood for death in comparison to placebo where typical antipsychotic drugs were used.
The authors assessed the evidence for high death rates from atypical antipsychotic medications for patients who have dementia. The data sources were obtained from Cochrane Controlled Trials Register, MEDLINE, and meetings and presentations.
A large sample size is used hence the findings could be generalized. There a total of 5,101 participants
Some very old data materials from the 1960s were used which may not be relevant for use today
High level
Step 2: History and purpose of research question
Every antipsychotic drug has warnings of increased mortality for elderly patients (Schneider, Dagerman & Insel, 2012). Antipsychotic medications are broadly utilized in managing psychological and behavioural symptoms in dementia in spite of concerns as regards their safety (Ballard et al., 2011; Piersanti et al., 2014). Compared to typical or conventional antipsychotic drugs, atypical antipsychotic drugs are linked to a statistically significant rise in the likelihood of mortality for older men and women who have dementia (Haddad & Sharma, 2012).
The purpose of the research question is to find out whether the use of typical antipsychotic medication, which is the intervention, results in less mortality rates than atypical antipsychotic medication, which is the comparison group, in elderly patients who have dementia and psychosis.
Step 3: Strengths and weaknesses of existing literature
The strengths of the existing literature is that there are studies which focus mainly on the atypical antipsychotics and others that focus mainly in typical/conventional antipsychotics and their correlation with mortality. The weakness of the existing literature is that there are no studies that compare typical antipsychotics and atypical antipsychotics on the rates of mortality on elderly patients with dementia and psychosis (Rochon et al., 2013).
Step 4: Gap in current literature
At the moment, the gap in current literature is that there are no studies which have focused specifically on the association of atypical and typical antipsychotic medications on the rates of mortality among the older adults who have dementia.
Want help to write your Essay or Assignments? Click here
Conclusion
In conclusion, the PICO question for the research study is as follows: In elderly patients who have dementia and psychosis (P), does treatment with typical antipsychotics (I) or atypical antipsychotics (C) result in less mortality (O). The purpose of the research question is to find out whether the use of typical antipsychotic medication results in less mortality rates than atypical antipsychotic medication in elderly patients who have dementia and psychosis. The resources used to find articles included electronic databases research, relevant books, and reputable journals. The search terms that were utilized include dementia, mortality, psychosis, atypical antipsychotics, and typical psychotics.
References
Ballard, C., Creese, B., Corbett, A., & Aarsland, D. (2011). Atypical antipsychotics for the treatment of behavioural and psychological symptoms in dementia, with a particular focus on longer term outcomes and mortality. Expert Opinion on Drug Safety, 10(1): 35-43
Piersanti, M., Capannolo, M., Turchetti, M., Serroni, N., De Berardis, D., Evangelista, P., Costantini, P., Orsini, A., Rossi, A., & Maggio, R. (2014). Increase in mortality rate in patients with dementia treated with atypical antipsychotics: A cohort study in outpatients in Central Italy. Riv Psichiatr, 49(1): 34-40.
Rochon, P. A., Gruneir, A., Gill, S. S., Wu, W., Fischer, H. D., Bronskill, S. E., & … Gurwitz, J. H. (2013). Older Men with Dementia Are at Greater Risk than Women of Serious Events After Initiating Antipsychotic Therapy. Journal of the American Geriatrics Society, 61(1), 55-61. doi:10.1111/jgs.12061
Schneider, L. S., Dagerman, K. S., & Insel, P. (2012). Risk of death with atypical antipsychotic drug treatment for dementia – Meta-analysis of randomized placebo-controlled trials, JAMA, Journal of the American Medical Association, 294(15): 1934-1943
Want help to write your Essay or Assignments? Click here
Want help to write your Essay or Assignments? Click here
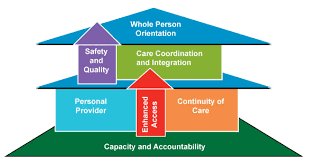
The patient-centered medical home model
The chronic care model refers to an organizational approach through which people suffering from chronic diseases can receive care in the primary care settings. It is population-based. Moreover, it creates supportive, evidence-based, and practical interactions between the activated, informed patient and proactive, and prepared practice team.
This model identifies some vital healthcare system elements which promote care for chronic diseases that is high-quality. Within the elements, there are particular change concepts, which are used by the team to guide the improvement efforts. The care redesign processes applied agree to the change concepts.
In the same way, the aim of the patient-centered medical home is ensuring that the patients receive better care (Varkey, 2010). The model focuses more on patient needs. Some of the aspects through which care access can be improved include increased communication between the patients and providers through telephone and email, and extending the office hours. The elements of the chronic care model increase care coordination as each contributes in its own way.
One of the goals of the patient-centered medical home is also increasing care coordination. Moreover, the latter model aims to enhance the overall quality and reduce costs simultaneously (The Commonwealth Fund, 2009).
The patient-centered medical home model has a keen focus on the whole person, and different healthcare professionals participate in the care provision. There aspects are not focused on the chronic care model where attention is solely on the chronic disease. Similar to the chronic care model, the patient-centered medical home model integrated all health care aspects for overall health improvement. A unique characteristic of the patient-centered medical homes is that patients seek care from personal physicians who lead care teams within the medical practice (National Business Coalition on Health & National Health Leadership Council, 2010).
Want help to write your Essay or Assignments? Click here
Elements that are most significant for achieving safety and quality goals
The patient-centered medical home model
This model also has some elements that promote achievement of its set goals. These are physician-led practice, whole-person orientation, coordinated and integrated care, access, and focus on safety and quality. These elements have to interact for the care being provided to be relevant. Same as the chronic care model, evidence-based medicine is given a lot of emphasis as it helps improve the patient outcomes. Moreover, the care team has to offer comprehensive care that is both coordinated and integrated (Institute for Healthcare Improvement, n.d.).
Chronic care model
This model identifies the cardinal elements that every healthcare system should have for high-quality care for chronic diseases to be realized. The elements are as follows; clinical information systems, decision support, delivery system design, self-management support, health system, and community. Under each element, there are evidence-based change concepts and in combination, they foster interactions that are productive and meaningful between informed patients that are very active in their health and well-being and providers with expertise and resources.
Based on this model, these elements should all interact for chronic diseases to be managed and prevented effectively. In essence, the factors in the community that contribute to chronic diseases should be addressed and measures taken to promote safer communities (Varkey, 2010). In addition, patients should engage in self-care and management; healthcare delivery should be safe, personalized, and high-quality; the best decisions should be made for better care provision; and the clinical side should also be effective.
As such, chronic diseases can be prevented and managed appropriately. All the elements of this model are important for safety and quality goals. Each of them has a cardinal contribution, and ignoring any would result to inefficiencies.
Want help to write your Essay or Assignments? Click here
Structuring the models to achieve the best medical outcomes for individual patients at the lowest cost to society
In relation to the chronic care model, the organizations being created should be committed to offering high quality and safe care. Basically, the business plan of the health system should reflect a dedication to applying the model across the organization. Moreover, the clinical leaders should ever be dedicated and visible members whose roles performance should be perfect. Again, the community resources should be mobilized so that the patients’ needs can be met. As a result, the chronically ill patients can be kept active, involved, and supported.
Moreover, it is necessary that the patients are prepared and empowered to as to participate in their healthcare. The delivery system design should assure self-management support and effective, efficient care. Birenbaum (2011) indicated that the decision support should promote care that agrees to patient preferences and scientific data. In relation to the clinical information systems, data should be organized to promote effective and efficient care (Varkey, 2010).
For the patient-centered medical home model to be effective, the team of providers have to cooperate. In addition, there has to be payment reform and health information technology. Considering that medical homes might be virtual or physical network of services and providers, there has to be health information technology that can facilitate information sharing and communication among providers. In addition, the providers receive financial incentives that enables them focus on quality as opposed to volume.
References
Birenbaum, A. (2011). Remaking chronic care in the age of health care reform: Changes for lower cost, higher quality treatment. Santa Barbara, Calif: Praeger.
National Business Coalition on Health, & National Health Leadership Council. (2010). Patient-centered medical home: Has the time come? : National Health Leadership Council, Portland, ME, June 22-24, 2010. Washington, D.C: National Business Coalition on Health.
Want help to write your Essay or Assignments? Click here
Abuse and Neglect
Every individual has the right to live safely and free from abuse and neglect. However, it is not always that every person lives this kind of life. People often fall into situations where they are vulnerable to abuse and neglect. It is important to note that abuse and neglect happens because people use power and intimidation to control another person’s life. Most of the cases of abuse and neglect are perpetrated by the people known to the victims.
However, strangers can also cause abuse to the people they do not know. The abuse that comes from the people known to the victims happens because the victim trusts their assailant. A feeling of trust and belief in the assailant makes it easy for victims to fall into abuse and trust quite easily.
There are many forms of abuse. Sexual abuses are acts that victims do not consent to, but are forced to participate in them. Physical abuses are in the form of assaults, slapping or hitting, just to mention a few forms. There is psychological abuse, which is in form of emotional abuse and verbal abuse, controlling the victim and threatening the person. Domestic abuse comes from a family member or relative. A victim can be abused through discrimination.
This kind of abuse causes unfair treatment of people from a different race, gender, religion, tribe, age or sexual orientation. People can also be abused financially, where one is forced to use or spend their money in ways that they do not feel are appropriate. Neglect is another form of abuse. This form of abuse means that the victim is left to suffer without proper care. In other words, when one fails to receive what they really need from their primary care giver, they are said to be neglected (NHS 2015).
Want help to write your Essay or Assignments? Click here
Task 1.1
The victims of abuse show certain signs that prove they are in an abusive relationship. One appears withdrawn and quiet. It is important to note that even for the people who are quiet, there is a form of withdrawal that is beyond the normal. The victims could become angry and aggressive, even in situations that do not require such emotions. In the case of John, mentioned in this case study, a victim can become unkempt and dirty.
In some extreme cases, victims have bruises, wounds and scars, to serve as proof that they are in an abusive relationship (CDC 2015). People like John have no power to stand up for themselves and fight back. This makes them vulnerable to harm inflicted by others.
Task 1.2
There are several factors that can lead to people becoming victims of abuse and neglect. Disability can cause a victim to suffer issues of neglect and abuse. This is because they have no power or capacity to do much for themselves. Secondly, the victims of abuse lack the capacity to understand their situation. For instance, a child has no capacity to comprehend what goes on in their home. This can cause the parents to be abusive to the child, knowing that the child lacks power to do anything about it.
The third factor that can cause people to become victims of abuse and neglect is the lack of physical, emotional or financial strength. For instance, a married woman who has no financial capacity to leave her abusive e spouse can become a victim of domestic abuse. In addition, a woman lacks the physical strength to fight a man, which means that she could become a victim of abuse (Kleinman 2015).
Task 1.3
Child abuse and violence against these young ones has dated back to the times before civilization ever took place. The culture and socially acceptable norms guide parents and guardians on the best way to bring up their children (Sperry and Widom 2013). One culture could advocate for disciplining the child by speaking and withdrawing privileges. Another culture believes that children need to be beaten, in order to instill discipline. Different cultures have different acceptable forms of parenting. The culture of a people serves as a source of beliefs and behavior and the concepts of how people should conduct themselves.
The diminishing status of the child in the parent-child relationship (WHO 2014) has affected the trust that should exist between children and their parents. Stalker and McArthur (2012) explain that social factors such as poverty can lead to abuse and neglect. Another social factor that can lead to abuse and neglect is social exclusion (Pillemer, Burnes, Riffin and Lachs 2016). The society tends to keep away from private issues. This forces many cases of domestic abuse to go unreported. Most people tend to argue that personal issues are not communal, which means that the victim suffers alone. Often, the society has the capacity to help the person, but people keep away from such matters for the fear of becoming victims.
M1
In response to the concern presented to the manager by Tina, the manager can take the responsibility by calling the parents to a meeting. One of the ideas to have in mind is that the manager has a role to play in the life of every child that comes into their facility. The manager can act as the guardian of the child by asking the parents to speak with a counselor about their issues.
This will help them to work on their frustrations, which they do not have to pass out on a three year old child. Secondly, the counselor can also call child social workers in case she sees that her approach is not yielding any result. A child social worker as well as a children advocate can help the manager to address the issue by having the child placed in foster care.
D1
Change means transforming practices that tend to be harmful to a vulnerable person. It is very important for organizations to change their practices. Many organizations can change certain unacceptable regulations and shape norms and new systems that promote health and safety. Another strategy that the nursery can use is to work with policy makers to give their suggestions and views about the issues that children go through in abusive situations. Policy makers can discuss and approve health and safety policies that protect the vulnerable groups from abuse and neglect (Promising Practice Network 2014).
Task 2.1
There are legislations that protect children and vulnerable people from abuse. The Care Act of 2014 places a general duty on the local authority to promote general wellbeing of individuals. The wellbeing of a person covers their physical and mental health, as well as their emotional well being. In addition, the local authority is mandated to ensure that the personal dignity of an individual is upheld, which means that people have to respect each other despite their age or gender.
This act protects the individual from abuse and neglect. The strength of this legislation is that it gives the local authority the capacity to ensure the individual has their wellbeing protected. There is the Safeguarding Vulnerable Groups Act 2006 and the Protection of Freedom Bills. This Act was passed to help avoid harm or risk of harm to children or the vulnerable adults. It prevents the people who are unsuitable to work with these vulnerable people (SCIE 2013).
Want help to write your Essay or Assignments? Click here
Task 2.2
There are professionals who deal with issues of abuse. Although many people tend to shy away from reporting child abuse cases. The fear that many people feel is that they will be breaking up a home. Others fear that the violent persons might start attacking them if they learn of the role they played in breaking a cycle of abuse. Another fear is that the report will not make a difference in the life of a child. However, it is better to be safe when it comes to the issue of a child. It is unfortunate that most people would rather be quiet about an abusive home than be involved (Committee on Child Maltreatment Research 2014).
The professionals that can be involved are child care providers and social workers. Child care providers could be in the setting of a school or a hospital. Observation serves as one of the best way to know a child who is abused. It is difficult for a child to hide their emotions and fears. Children who are victims of an abuse will often show fear on their faces. This is one of the signs to look out for in a child who is in an abusive home. Social workers are the agents who intervene in the cases of abused children. The social worker can take and place a child in a different home once the case of abuse has been proven to be true.
M2
It is important to understand the consequences of child abuse and neglect. A child who grows in such an environment is prone to physical and mental growth. In addition, a child can become hopeless about having a good life. A child living in an abusive home can have a very low self-esteem. The cognitive development of a child in an abusive home can be delayed. When these children are compared to their peers, these children often grow slower (Powell and Uppal 2012). In addition, their academic performance is poor.
The government can work with social workers and institutions of learning to reach out to the children who are in abusive homes. The fact is that every child has a right to having a good life. A good life, in this case, does not mean that the child has material property provided to them. The basic needs that are very important to a child are food, shelter, clothing and love. Children need a lot of love for them to cultivate a positive attitude towards life. The government should ensure that every child receives these things.
When one considers the reaction of the mother, it is clear that she avoids talking about the issues she faces. One of the strategies that can help the manager to deal with the issue of abuse is to separate the mother from the source of the harm. It looks like the mother is in a place where the issues she faces instil fear in her, to the extent that she is not able to defend her own son. The manager can ask the local authority to provide the mother and the child with some form of protection until their case is solved by the social workers who work with children.
The manager can work with the mother to understand the reason as to why she is reluctant to speak about the bruises that Tina reports to the office. From the mother’s point of view, the manager can address the issue armed with information from the guardian of the child. In addition, the manager can speak with the child so as to understand the situation in which they live. A child, at the age of John, does not know how to lie. This means that the information that John gives to the manager can be dependable. This information can be used by the manager and the concern parties to ensure that John gets a change of environment, which will ensure his own safety and health are protected.
D2
The nursery needs to recognize that their staff members need to understand how to handle cases of child abuse. The manager can organize training for their staff members. This will increase their knowledge on how to handle issues such as John’s within the school setting. The manager can organize with child-related organizations to address issues of handling children from abusive environments. These training workshops can employ the use of a trained social worker to pass information to the other staff members about recognizing and addressing the signs of child abuse. A professional in children’s issues can also help the staff members to know how to communicate with children.
Task 3.1
One strategy to use in addressing child abuse in the community is fostering relationships, coalitions and networks with different child organizations (CDC 2015). This means that the community together with other organizations helps address this issue. In this case study, John is a three year old boy. His care giver, Tina notices that he comes to school dirty and unkempt. Tina observes that John is not interacting well with his peers. The care giver also notices that the boy has bruises on his arms. When the care giver asks the mother, she evades this discussion. Tina and the manager can seek help from the other members of the community. This means that the care givers can use the other community members to face this issue.
The area networks that can be created to help these children. One of the arms of this network is the local authority. In the case of John, he has attended school with bruises. This means that John has been a victim of physical violence. The local authority can investigate the family from which John comes from. It is illegal to inflict harm on a child. As such, the local authority should confront this family in order to protect the child from such abuse.
There are religious groups that can work with the nursery to help the child and the family to heal from this abuse. It is important to understand the religious group with which John and his family associate. The hospital and healthcare providers can also form part of the network that deals with child abuse and neglect. It is important to involve the Ministries that deal with the welfare of Children. All these bodies alongside the nursery can assist John and his mother through the situations they have to face.
Want help to write your Essay or Assignments? Click here
Task 3.2
There is a disadvantage to engaging one approach. The adoption of one approach means that the problem is dealt with at the individual level. This means that the broader scale will remain the same. It is important to change the societal norms and systems. It will therefore mean that the settings in the society will have to go through changes or instance; the people have to learn the effects of child abuse on the child as well as the society. For instance, a child from an abusive environment tends to grow depressed and with a negative image of life. As such, these people tend to be poor performers even at the workplace. If the society can change such issues, then it means that the community benefits in a more profitable way.
It is important to combine approaches, which will address the child abuse issue. The community needs to strengthen the individual’s knowledge and skill in combating child abuse cases. This could include demonstrating to individuals how to promote safety within schools and the society. For instance, it is important to know how to deal with a parent who argues that their disciplining methods are not abusive, yet their child has bruises on their body.
The promotion of community education (Powell and Uppal 2012) in such matters helps the entire community know and use their acquired knowledge to deal with these issues. This strategy uses reaching groups to educate the community. These groups provide the community with information and resources on how to promote health and safety for the vulnerable groups in the society (Promising Practice Network 2014).
Task 3.3
In many cases, child abuse cases happen to children who cannot stand up for themselves despite the pains they face (WHO 2014). Many of the children from abusive environments have to live with threats from their assailants. Often, they are forced to keep quiet about their ordeals. The assailants often threaten the victims to remaining quiet about their attacks. As such, children fear the consequences of sharing their issues with a person who is not their primary care giver. The staff members need to learn how to address these children, giving them hope and assurance of their safety. This means that the nursery can train its staff members on how to handle young children who live in fear.
There is need to constantly review and update the practices that are used in protecting children from abuse. The government and the policy makers need to create collaborations with people who work with children. This will ensure that every concern party makes a significant contribution to the policies and laws that protect children from abuse. It is the responsibility of the community to ensure that every case of child abuse reaches the relevant authority. This means that the community can work together to protect the children and the vulnerable people from abuse and neglect.
In order for the community to understand how they can address the issues of child abuse and neglect, they need to be equipped with information and resources in this field. Community social and health workers can organize programs that teach the community members on the measures to take when they learn of a case of child abuse. In addition, parents can take education and training programs to show them how to handle themselves in a case of child abuse. People need to grow out of the fear that their intervention can bring about destruction in a family. Protecting a vulnerable person from abuse gives the victim a chance to have a better life.
Conclusion
The cases of child abuse have been in existence in our society for a very long time. It is important to know the organizations and the networks that one can use to ensure that these children grow in safe and healthy environments. The groups that are susceptible to abuse need protection from assailants. The local law enforcement needs to get involved in the systems that help ease the pain for these people.
In order to help a victim of abuse and or neglect, it is important t understand the type of abuse they go through. The signs of abuse are not very obvious, especially when physical evidence is absent. It is therefore important to have knowledge on all the signs of abuse, before any assistance can be rendered to the victims.
Pillener, K., Burnes, D., Riffin, C., and Lachs, M. 2016. ‘Elder Abuse: Global Situation, Risk Factors and Prevention Strategies.’ The Gerontologist 56(2): S194-S205.
Powell, J. and Uppal, E., 2012. Safeguarding Babies and Young Children: A Guide for Early Years Professionals, Berkshire, McGraw Hill Education.
Sperry D. M. and Widom, C. S. 2013. ‘Child Abuse and Neglect, Social Support, and Psychopathology in Adulthood: A Prospective Investigation.’ Child Abuse and Neglect Vol 37(6): 415-425.
Stalker, K. and McArthur, K., 2012. ‘Child Abuse, Child Protection and Disabled Children: A Review of Recent Research.’ Child Abuse Review Vol 21 (1): 24-40.