Get a Custom Essay Paper that meets your expectations by clicking ORDER
Fibroids
Order Instructions:
Develop a 30-minute presentation, with detailed speaker notes, on Fibroids.
Analyze the etiology, pathophysiology, and general clinical manifestation of symptoms of the disease based on relevant literature.
Consider how age or overall health status might alter the normal clinical manifestation of the disease.
Evaluate the patient’s overall social and medical history, clinical symptoms, and clinical assessment from the perspective of the previously cited literature.
Evaluate the diagnostic work-up and clinical findings, including a rationale for each diagnostic test and expected findings, and recommend a diagnosis based on the findings.
Develop a plan of care based on diagnosis, including age-appropriate modifications of proposed therapy and dose modifications based on clinical guidelines.
Include medications, assistive therapies, and specific limitations of activities.
Address any age-appropriate modifications of proposed therapy or dosage modifications.
Analyze the potential complications of care and any possible side effects of medication based on literature that includes instructions for notification of the clinician.
Create a patient education plan that shows understanding of the patient’s developmental age, sexuality, health literacy, socioeconomic status, cultural sensitivity, and health belief models.
Analyze current condition and how it may relate to underlying health issues, the proposed plan of care, and possible side effects or complications.
Include patient/family engagement in the plan of care using the teach-back method.
Analyze how the principles of Watson’s theory of human caring are integrated into the plan of care and patient education.
Conclude the presentation with a question-and-answer session (8 to 10 questions and answers).
Prepare a one-page summary as a handout for the other students. Reference needs to include UpToDate
Below is a partial answer to the above homework questions by one of our writers. If you are interested in a custom non plagiarized top quality answer, click order now to place your order.
Fibroids
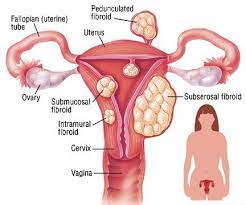
Fibroid are the most common tumors that affect women’s reproductive system. They are benign tumors that made of smooth muscle cells that grow in the uterus. Further, these tumors affect women in their reproductive and almost fifty percent of such women in their child bearing age have fibroids. Generally, thirty to seventy percent of women will develop fibroids at some point in their reproductive age (Stewart, 2017).
However, although fibroids are dangerous and cause disruption in women’s lives, they are not cancerous in nature and their development do not increase the risk of developing cancer. Additionally, the cause of fibroid development in the uterus remains remain unknown. Despite its cause being unknown, women with a family history of tumors, those who are obese, African American women, women who commence their periods early and those who are nulliparous are at risk of developing fibroids (Stewart, 2017).
Generally, the main symptoms indicating the presence of fibroids are heavy and prolonged bleeding, pain and discomfort in the pelvis and abdomen, urinary tract and bowel problems such as frequency in passing urine and incontinence, infertility issues and pain during menses and sexual intercourse. These presence of these symptoms and there severity will depend on the size and location of the fibroid.
When one visits a doctor, a thorough diagnosis has to be so as to exclude the possibility of other tumors, which may even be cancerous (Stewart, Barbieri, Goff, Falcone, & Falk, 2015). A history of the patient is taken including the manifested symptoms, the obstetric history and medical history. After that the patient is subjected to a physical examination which involves palpation of the abdomen. A pelvic ultrasound is the used to image the reproduction structure. This is the basic method used for the diagnosis of fibroids. In other cases, Magnetic Resonance Imaging is done in complex cases (Stewart, 2017)…..
Get a Custom Essay Paper that meets your expectations by clicking ORDER
Best-practices for providing health care to a nation and why
Want help to write your Essay or Assignments? Click here
Topic: Best-practices for providing health care to a nation and why
Instructions:
What are some of the “best-practices” for providing health care to a nation and why?
Improving quality of care and patient safety practices can strengthen health care delivery systems, improve health sector performance, and accelerate attainment of health-related Sustainability Development Goals.
We can write this or a similar paper for you! Simply fill the order form!
US federal and state governments impact health policy
Want help to write your Essay or Assignments? Click here
US federal and state governments impact health policy
Order Instructions:
First discussion:
You are an acute care nurse practitioner who works in an urban emergency room (ER). You see many people who come to the ER who have overdosed (OD) on heroin. Emergency medical services personnel may administer a drug that might reverse the overdose such as naloxone (Narcan). You may see three ODs during each 12-hour shift; some of these patients are admitted to the hospital, and others are sent home with a consultation for psychiatric follow-up. You are becoming hardened to the issue and have begun to question what you can do to address this epidemic.
Answer 1-2 of the following questions below
You hear that the state health director is convening a task force. List four actions you can take to be invited to participate in this task force.
Want help to write your Essay or Assignments? Click here
Which other healthcare professionals should be included in the task force?
Second discussion post: needs to be 200 words plus reference.
How does the structure of the US federal and state governments impact health policy? How do elected officials play a role in the development of policy and its continued movement?
We can write this or a similar paper for you! Simply fill the order form!
We can write this or a similar paper for you! Simply fill the order form!
Koplan on Global Health
Order Instructions:
Koplan on Global Health, (2009) wrote an opinion article in Lancet stating:
The need for a commonly used and accepted definition [of global health extends beyond semantics. Without an established definition, a shorthand term such as global-health might obscure important differences in philosophy, strategies, and priorities for action between physicians, researchers, funders, the media, and the general public. Perhaps more importantly, if we do not clearly define what we mean by global health, we cannot possibly reach agreement about what we are trying to achieve, the approaches we are to take, the skills that are needed, and the way that we should use resources (p. 1993)
Koplan on Global Health
We can write this or a similar paper for you! Simply fill the order form!
Koplan et al. (2009) offered the following definition of global health: “…global health is an area for study, research, and practice that places a priority on improving health and achieving equity in health for all people worldwide” (p. 1995). In Koplan et al.’s (2009) commentary, they offered a table distinguishing global health from international health and public health.
On the other hand, Margaret Bentley and her colleagues rebutted Koplan et al.’s position in a 2010 edition of the Lancet and believes global health and public health are indistinguishable.
Do you think global health and public health are 2 distinct disciplines or are they indistinguishable?
In your response, state your position supported by evidence while discussing both sides of the argument.
We can write this or a similar paper for you! Simply fill the order form!
Want help to write your Essay or Assignments? Click here
Determinants of health and ways they impact persons health
Introduction
To improve the health status of the community, there is need to reduce the health inequalities. This is only achieved by understanding factors that promote as well as protect health of the community, which are commonly referred to as determinants of health (Fane & Ward, 2014). These determinants are categorised into social, cultural and economic factors.
This is important because despite the fact that the USA government is spending fortune in medical care, the health outcomes still remains low than most of the developed countries. In fact, the USA IS ranked the 34th in infant mortality in the world (Potter, Trussell, & Moreau, 2009).
However, it is possible to envision the more promising end of this medical story if number of strategies are employed to understand as well as promoting the health of the community. This is achieved through analysis of health determinants as outlined by logic models (Blanchard et al., 2013).
These models are important because they are oversimplified and approximate, thus helping the identification of complex interplay, which would be important in taking action to improve the health of the population, which are developed by the new framework of health goals for USA, commonly referred to as “ Healthy People 2020 (Fane & Ward, 2014).”
This paper summarizes the main sociocultural and economic determinants of health and ways they impact the health of a person, leading to inequalities. Understanding these determinants is important because it helps improve the health of the community, thereby reducing healthcare inequalities. This aid in the identification of the specific areas for actions, which also facilitates the identification of the most feasible interventions that could aid promote quality care.
Want help to write your Essay or Assignments? Click here
Determinants of health
Evidence based study indicates that certain healthcare behaviours affects personal and community health. These includes behaviours such as smoking, poor nutrition, physical inactiveness, and excessive alcohol consumptions. Similarly, the amount of household income, educational achievement, ethnic background, employment and neighbourhoods also associated with profound effects of health (Perrin, 2013).
To start with, income and wealth determinants impact the health of a person. Research indicates that increased income improves the health outcomes. However, the relationship between health and income is not linear (Potter, Trussell, & Moreau, 2009). This is because money itself does not translate into good health. Instead, wealth is generally considered to give someone position within the society, which makes them, have better access to better economic opportunities (Salt, 2014).
This makes them live in healthy and safe communities, with better equipped facilities. Additionally, they are able to afford health insurance, and thus can access health more easily. Most have great amount of wealth and assets such as savings, low debt and high amount of savings that can be disposed to meet the health demands of the person where necessary (Blanchard et al., 2013).
Conversely, poor people are restricted to these amenities and are often exposed to environments that are health damaging. They lack sufficient amenities such as recreational facilities, grocery stores or even health care facilities (Fane & Ward, 2014). These people will lack social supports or relationships, have poor self-esteem, lack sense of control and are more likely to suffer from chronic diseases and acute stress. This impact is particularly vital in children and infants. Low income is associated with increased infant and childhood mortality.
It is also suggested that the hardship and economic deprivation in childhood significantly affect the adult health (Fane & Ward, 2014). Thus, children in low income households are more likely to suffer from poor nutrition, which results to health complications in their adult life including obesity, cancer, mental health, and cardiovascular diseases. This forms a vicious cycle of poverty and health (Potter, Trussell, & Moreau, 2009).
Want help to write your Essay or Assignments? Click here
The link between socioeconomic factors and health is clearer. However, the communities in which people live also influences their health. Literature indicates that people living in poor neighbourhoods report higher mortality rates, high incidences of chronic diseases and poorer health standards as compared with people living in safer neighbourhoods (Potter, Trussell, & Moreau, 2009). One study conducted in Wake County, North Carolina indicated that people living in poorer neighbourhoods reported higher incidences of pre-term birth, greater levels of depression, high level of teen pregnancy and increased resistance and disorders among the adolescents (Fane & Ward, 2014).
Additionally, different neighbourhoods makes it difficult to access healthy food, availability of parks and sidewalks and open spaces where people can exercise. The proximity of the people to environmental hazards also influences the quality of care (Diaz de León-Castañeda, RamÃrez-Fernández, & Pinzon Florez, 2013).
Housing also influences the health being of an individual. Living in houses that are poorly ventilated, damp, overcrowded or with poor waste disposal strategies are associated with increased diseases, communicable infections and other preventive diseases (Salt, 2014). Housing structures are very important as people spend approximately 90% of their time within their home, and thus poor housing can put people at risk of developing health complications due exposure to environmental hazards (Fane & Ward, 2014).
Additionally, overcrowding increases the risks of transmitting infectious diseases such as tuberculosis as well as other respiratory diseases (Blanchard et al., 2013). It could lead to more healthcare complication in events of pandemics such as virulent influenza. Research estimated that low income households live in overcrowded conditions, where more than 70,000 housing units in USA are overcrowded (Potter, Trussell, & Moreau, 2009). The issue is more complicated with most people facing foreclosures which is associated with the downturn of the economy. This accelerates the risk of sharing housing, and doubling up of people with their families and friends (Cai & McAdam-Marx, 2013).
Want help to write your Essay or Assignments? Click here
Academic achievement is strongly correlated with increased lifespan. Generally, people with less education are associated with more chronic complications and their life expectancies are shorter as compared with people with higher level of education (Blanchard et al., 2013). This is indicated by the healthcare study, where adults who have finished high school are more likely to have better health outcomes as compared with dropouts (Salt, 2014). In the USA, the ager adjusted mortality of people who dropped out of high school is two folds higher than those who completed their education.
These people are more likely to suffer from chronic and acute healthcare complications such as hypertension, stroke, diabetes, asthma, ulcers and emphysema. On average, it is estimated that the college graduates live five years longer as compared to those who failed to complete high school education (Diaz de León-Castañeda, RamÃrez-Fernández, & Pinzon Florez, 2013).
Research indicates that education achievement and health are not only correlated at personal level but also in their future generation. For example, maternal education is associated with better health for the children. Similarly, children born by high school dropout’s parents are two folds likely to suffer from premature death. Educated mothers’ infant mortality rates are considerably lower than uneducated parents. This is because educational achievements, wealth and health are interrelated, and have significant impacts on person’s health.
Another important health determinant is social exclusion, which is often associated with poverty. Social exclusion is associated with huge impacts in health such as premature deaths. Absolute poverty results to lack of basic materials, and is still rampant in developed countries (Salt, 2014). Most of the unemployed people, ethnic groups, refugees, homeless and the disabled are often socially excluded. This denies them the opportunity to access decent living opportunities such as education, housing, transport or even the ability to participate in various activities of the lives that makes them participate fully. This exclusion and being treated as lesser beings leads to health complications (Cai & McAdam-Marx, 2013).
Want help to write your Essay or Assignments? Click here
The social exclusions occurs inform of racism, discrimination, hostility, stigmatization as well as unemployment. These denies people their ability to participate in educative training, prevention programs or even accessing potential beneficial healthcare capacities. These issues are socially as well as psychologically damaging, and can have detrimental effects to these discriminated people (Pegram & Bloomfield, 2013).
The longer these people live in prisons, psychiatric facilities and children’s homes, and the more likelihood of them to suffer from a wide range of disorders. These incidences are also associated with increased risk of divorce, addictions and disabilities. Research indicates that people with strong family relations have better health outcomes. For instance, the highest incidences of mental illness are from single parent families (Pegram & Bloomfield, 2013).
Addiction is a public health issue of concern as it is associated with social breakdown, which worsens the issue of healthcare disparities. Addiction in this context refers to overreliance of drug use such as alcohol and cigarrette smoking. This is associated with increased mortality associated with suicides, injuries and poisoning. Although unclear, cultural values and beliefs tend to influence the quality of care (Salt, 2014).
This includes activities such as religious values that prohibits people from seeking medical assistance. Other determinants includes population based healthcare facilities as well as services. These includes activities such as sewerage and water to ensure that people’s health is maintained. The extent of funding of these activities dictates the level of the maintenance of this infrastructure, their developments and also usages.
Want help to write your Essay or Assignments? Click here
Ways the determinants of health impact people’s health
Most of the social factors mentioned above are described to have both interactive and independent effects. For instance, people with high level of incomes are more likely to have achieved higher education. They are also more likely to have more opportunities to live in safe, standard and healthy environments. Their neighbourhoods are more likely to be secure, thus promoting physical activeness. They are also able to purchase organic food as compared to those with low income households. These people are also more likely to have medical cover, which facilitates access to quality care (Cai & McAdam-Marx, 2013).
Conversely, people living with poverty are more likely to have lower education achievement, indicating that they are most likely unemployed. They will often live in substandard housing, putting them at risk of communicable diseases due to overcrowding effects and poor sanitation (Cai & McAdam-Marx, 2013). These people lack enough resources to purchase quality foods, hence depends mainly with fast food, increasing the risk of obesity. These people are more likely to engage in risky behaviours such as drug abuse and prostitutions, putting them at greater risk. This makes them experience higher levels of stress as compared with their counterparts (Pegram & Bloomfield, 2013).
Want help to write your Essay or Assignments? Click here
Whereas most of these factors are interconnected as described above, there is growing evidence that these factors independently determine the health of the people. For instance, in the USA, the health status of all ethnic communities decreases as income level decreases. It is reported that people with 100% federal poverty guidelines (FPG) reports the worse health as compared to people in other income level (Pegram & Bloomfield, 2013). However, within each income levels, specific communities have worse health outcome as compared with others.
For instance, the African American normally reports poor healthcare outcomes as compares to the Hispanics and non-Hispanics white (Cai & McAdam-Marx, 2013). These marked differences across the ethnic communities are observed in other determinants of health. Therefore, to effectively reduce the increased healthcare disparities, issues such as accessibility of educations, standard housing, safe living as well as working environments, healthcare facilities and all other opportunities that facilitate the healthy living of the community must be addressed (Diaz de León-Castañeda, RamÃrez-Fernández, & Pinzon Florez, 2013).
Conclusion
As indicated, it is evident that there is strong correlation between the health and people’s incomes and way of life including community environment, educational achievement, and ethnicity and housing conditions. It is indicated that those people with higher incomes, higher education achievement and those living in a health as well as safe environments have been associated with longer life expectancies and are associated with better health outcomes. Conversely, people with lower education levels, living below poverty line, substandard housing and those in poor neighbourhoods have poor health outcomes. This is attributable to the fact that these lack sufficient resources to treat even the preventable diseases. This translates to increased health disparities among the various ethnic groups.
References
Blanchard, C., Gibbs, M., Narle, G., & Brookes, C. (2013). Learning from communities in the USA and England to promote equity and address the social determinants of health. Global Health Promotion, 20(4 Suppl), 104-112. http://dx.doi.org/10.1177/1757975913501006
Cai, B., & McAdam-Marx, C. (2013). The determinants of antihypertensive use and expenditure in patients with hypertension in the USA. Journal Of Pharmaceutical Health Services Research, 5(1), 11-18. http://dx.doi.org/10.1111/jphs.12041
Diaz de León-Castañeda, C., RamÃrez-Fernández, D., & Pinzon Florez, C. (2013). Compared Analysis of Inequalities in Health and Influence of Social Determinants of Health in Cuba and USA. Value In Health, 16(7), A711. http://dx.doi.org/10.1016/j.jval.2013.08.2189
Fane, J., & Ward, P. (2014). How can we increase children’s understanding of the social determinants of health? Why charitable drives in schools reinforce individualism, responsibilisation and inequity. Critical Public Health, 1-9. http://dx.doi.org/10.1080/09581596.2014.935703
Pegram, A., & Bloomfield, J. (2013). The importance of measuring blood pressure in mental health care. Mental Health Practice, 16(6), 33-36. http://dx.doi.org/10.7748/mhp2013.03.16.6.33.e849
Potter, J., Trussell, J., & Moreau, C. (2009). Trends and determinants of reproductive health service use among young women in the USA. Human Reproduction, 24(12), 3010-3018. http://dx.doi.org/10.1093/humrep/dep333
Over the past few years, new cases of people with diabetes have been on the rise. The increased incidence has been attributed to factors such as overweight, obesity and unhealthy lifestyles. A health promotion program was planned and carried out with the principle objective of improving the health through health education, encouraging people to embrace healthy lifestyles and minimizing complications associated with diabetes type 2( Saunders & Evans 2012). After the health promotion program, information from the target group gathered through structured questionnaires and focused group discussions, so us to help evaluate whether the program added any value to their lives (Saunders & Evans 2012).
The diabetes health program was aimed at reaching five hundred individuals between the age of 28 and 50 years in the community (Saunders & Evans 2012). Unfortunately, only a few individuals of the target group turned up. Activities which were carried out included health education on predisposing factors treatment, complications, and screening of diabetes. However, not all the activities that were designed reached the target group, and this made the stakeholders de-satisfied with the project. The activities which were intended were not all implemented since there was poor turn up of people.
Immediately after the health promotion program, new cases of people with diabetes type two were being reported and also those with uncontrolled blood sugar were still noted in various healthcare settings. These results clearly indicated that the objectives of the health program were partially met. Nevertheless, this could have been attributed to external factors such as cultural background which hindered individuals from taking certain foods or low economic status which limited people from accessing medical services and buying materials for blood-sugar monitoring (Bauman & Nutbeam, 2013).
Since the program was unsuccessful, new strategies were raised so as to ensure the success of future programs. This would involve coming up with better modes of communication to the individuals such as brochures and through television. This would help in adding weight to various messages and also acting as constant reminders on diabetes avoidance (Bauman & Nutbeam, 2013).
The case study is about a 5-year old child who is diagnosed with right ear infection. The patient’s mother reports that the child is very irritable, fatigued and have a fever for 102 F for the past 2 days. The mother also states that the child has been eating but has been drinking fluids only. The healthcare provider described the tympanic membrane (TM) as erythmatic, bulging with fluid levels and was dull.
Based on these clinical presentations, the differential diagnosis for this patient is Acute Otitis Media, Acute Otitis Media with effusion, Mastoiditis and foreign body in the ear (McCance, & Parkinson, 2010). From the clinical manifestation of fever, erythmatic TM, swollen TM and otalgia is an indicator that the patient is having bacterial infection in his right ear. The patient is not because the patient could be having swollen lymph nodes caused by immune response to the infection (CDC, 2016).
Add New Post
about:blankChange block type or styleChange text alignmentAdd titleFever Case Study
Fever
Case study 1: fever
The case study is about a 5-year old child who is diagnosed with right ear infection. The patient’s mother reports that the child is very irritable, fatigued and have a fever for 102 F for the past 2 days. The mother also states that the child has been eating but has been drinking fluids only. The healthcare provider described the tympanic membrane (TM) as erythmatic, bulging with fluid levels and was dull.
Based on these clinical presentations, the differential diagnosis for this patient is Acute Otitis Media, Acute Otitis Media with effusion, Mastoiditis and foreign body in the ear (McCance, & Parkinson, 2010). From the clinical manifestation of fever, erythmatic TM, swollen TM and otalgia is an indicator that the patient is having bacterial infection in his right ear. The patient is not because the patient could be having swollen lymph nodes caused by immune response to the infection (CDC, 2016).
Question 1: Fever is commonly considered to be triggered by viral or bacterial infection. The body has the ability to regulate its body temperature to maintain it at 37ºC. The hypothalamus –part of brain-helps control body temperature by triggering changes to the effectors such as muscles and sweat glands (McCance, & Parkinson, 2010). The temperature receptors in the human skin detect the external temperature that is transmitted to the hypothalamus.
This is the processing centre automatically trigger changes to effectors (muscles and glands). For instance, when it is too cold, the processing centre sends nerve impulses to skin where erector pilli muscles contract, causing skin hairs to erect and trap more warmth, reducing the heat loss, when heat is high, and skin muscles to relax causing hairs to lay down flat facilitating heat loss.
In addition, when it is too hot, the sweat glands in the skin secrete sweat on the surface that increases heat loss through evaporation, thereby cooling the body. Other responses include reducing blood flow to peripheral organs or increasing blood flow to the peripheral organs when it is cold, and inducing shivering (McCance & Parkinson, 2010).
Fever occurs if thermostat resets to higher temperature mainly due to an infection. When the bacteria invade the tissue, one of the immune system reactions is production of pyrogens. These chemicals are carried to the brain where they inhibit the heat sensing neurons while exciting the cold sensing neurons, these alterations of the temperature sensors makes the hypothalamus to trigger mechanism of raising temperature, which causes fever (Lieberthal et al. 2013).
Question 2: The clinical manifestation that indicates localized inflammatory response in this case study is erythema, fever, otalgia and swelling of the eardrum. The physiological factor associated with erythema is increased vasodilatation that increased blood flow to the infected area. This is mediated by release of inflammatory chemicals such as prostaglandins, histamine, and leukotrienes.
The physiological factor that caused swelling of the eardrum is increased permeability in order to increase fluid loss at the inflammation area (McCance, & Parkinson, 2010). This causes an increase mobility of the immune cells and also works as coagulation system that prevents spread of infection. The swelling is also associated with exudates behind the eardrum. Pain (otalgia) is associated with increased release of prostaglandins- chemical mediators that increases stimulation of pain receptors at the site of infection.
The physiological factor for fever is due to increased blood flow, which increases warmth in the infection site. The high levels of temperature increase production of the white blood cells. The increased blood flow is also secondary to release of chemical mediators such as histamine (Shaikh et al. 2011).
Question 3: A complete blood count (CBC) is important during clinical decision-making. This is because it provides information of relative different types of cells in the circulation system. In patients with bacterial infection, the white blood count is generally the most powerful piece of information from CBC. The CBC indicates elevated levels of WBC (leukocytosis).Bacterial infections are also associated with increased in neutrophil levels (polymorphonuclear cell) (McCance, & Parkinson, 2010).
These CBC findings are due to systemic responses where the epithelial cells in the middle ear release beta defensins whose main role is to stimulate production of pro-inflammatory cytokines that acts as chemo-attractants for mast cells, T cells, neutrophils and dendritic cells that will inhibit bacterial toxins directly. Therefore, the elevated levels of neutrophil and WBC is systemic response to bacterial infection in the middle ear (McCance & Parkinson, 2010).
Conclusion
Ear infections are most common infections in pediatric primary care settings. The infections are mainly caused by bacterial infection. The main goals of treatment are to manage clinical symptoms and to manage hearing loss. For bacterial infections, the child should be treated using Amoxicillin in the right dosages. Sometimes ear infections can heal without use of antibiotics. However, the ‘watch and wait’ approach should be only be applied for 48-72 hrs, if no improvements are reached, then the patient must be treated with appropriate antibiotics.
Lieberthal, A.S., Carroll,A.E., Chonmaitree ,T., et al.(2013).The diagnosis and management of acute otitis media. Pediatrics, 131:e964..
McCance, K. & Parkinson, C. (2010). Study guide for Pathophysiology, the biologic basis for disease in adults and children, sixth edition. St. Louis, Mo.: Mosby.
Shaikh, N., Hoberman, A., Kaleida ,P.H., et al. (2011).Otoscopic signs of otitis media. Pediatr Infect Dis J 30:822.
Want help to write your Essay or Assignments? Click hereRank Math https://www.bestessaywriters.com/?p=524398
Question 1: Fever is commonly considered to be triggered by viral or bacterial infection. The body has the ability to regulate its body temperature to maintain it at 37ºC. The hypothalamus –part of brain-helps control body temperature by triggering changes to the effectors such as muscles and sweat glands (McCance, & Parkinson, 2010). The temperature receptors in the human skin detect the external temperature that is transmitted to the hypothalamus.
This is the processing centre automatically trigger changes to effectors (muscles and glands). For instance, when it is too cold, the processing centre sends nerve impulses to skin where erector pilli muscles contract, causing skin hairs to erect and trap more warmth, reducing the heat loss, when heat is high, and skin muscles to relax causing hairs to lay down flat facilitating heat loss.
In addition, when it is too hot, the sweat glands in the skin secrete sweat on the surface that increases heat loss through evaporation, thereby cooling the body. Other responses include reducing blood flow to peripheral organs or increasing blood flow to the peripheral organs when it is cold, and inducing shivering (McCance & Parkinson, 2010).
Fever occurs if thermostat resets to higher temperature mainly due to an infection. When the bacteria invade the tissue, one of the immune system reactions is production of pyrogens. These chemicals are carried to the brain where they inhibit the heat sensing neurons while exciting the cold sensing neurons, these alterations of the temperature sensors makes the hypothalamus to trigger mechanism of raising temperature, which causes fever (Lieberthal et al. 2013).
Question 2: The clinical manifestation that indicates localized inflammatory response in this case study is erythema, fever, otalgia and swelling of the eardrum. The physiological factor associated with erythema is increased vasodilatation that increased blood flow to the infected area. This is mediated by release of inflammatory chemicals such as prostaglandins, histamine, and leukotrienes.
The physiological factor that caused swelling of the eardrum is increased permeability in order to increase fluid loss at the inflammation area (McCance, & Parkinson, 2010). This causes an increase mobility of the immune cells and also works as coagulation system that prevents spread of infection. The swelling is also associated with exudates behind the eardrum. Pain (otalgia) is associated with increased release of prostaglandins- chemical mediators that increases stimulation of pain receptors at the site of infection.
The physiological factor for fever is due to increased blood flow, which increases warmth in the infection site. The high levels of temperature increase production of the white blood cells. The increased blood flow is also secondary to release of chemical mediators such as histamine (Shaikh et al. 2011).
Question 3: A complete blood count (CBC) is important during clinical decision-making. This is because it provides information of relative different types of cells in the circulation system. In patients with bacterial infection, the white blood count is generally the most powerful piece of information from CBC. The CBC indicates elevated levels of WBC (leukocytosis).Bacterial infections are also associated with increased in neutrophil levels (polymorphonuclear cell) (McCance, & Parkinson, 2010).
These CBC findings are due to systemic responses where the epithelial cells in the middle ear release beta defensins whose main role is to stimulate production of pro-inflammatory cytokines that acts as chemo-attractants for mast cells, T cells, neutrophils and dendritic cells that will inhibit bacterial toxins directly. Therefore, the elevated levels of neutrophil and WBC is systemic response to bacterial infection in the middle ear (McCance & Parkinson, 2010).
Conclusion
Ear infections are most common infections in pediatric primary care settings. The infections are mainly caused by bacterial infection. The main goals of treatment are to manage clinical symptoms and to manage hearing loss. For bacterial infections, the child should be treated using Amoxicillin in the right dosages. Sometimes ear infections can heal without use of antibiotics. However, the ‘watch and wait’ approach should be only be applied for 48-72 hrs, if no improvements are reached, then the patient must be treated with appropriate antibiotics.
Lieberthal, A.S., Carroll,A.E., Chonmaitree ,T., et al.(2013).The diagnosis and management of acute otitis media. Pediatrics, 131:e964..
McCance, K. & Parkinson, C. (2010). Study guide for Pathophysiology, the biologic basis for disease in adults and children, sixth edition. St. Louis, Mo.: Mosby.
Shaikh, N., Hoberman, A., Kaleida ,P.H., et al. (2011).Otoscopic signs of otitis media. Pediatr Infect Dis J 30:822.
Want help to write your Essay or Assignments? Click here
Working in partnership in health and social care is a vital aspect. Partnership refers to a shared jointness and power, marked by respect for one another, divisions of roles, accountability and individual input. Different terms are used to define partnership including cooperation, shared learning, teamwork, participation and multi-disciplinary working. The staffs in healthcare have the responsibility to recognize the importance of promoting autonomy within the service users and the service providers.
They are not only expected to be attentive to their own roles but also learn to relate with each other’s within the within St Andrew’s healthcare facility. This is important particularly in the view of the unrest and cynicism observed in the NHS. Therefore, it is important for those concerned about their commitment in developing a mutual relationship for the good of the service users (Soni 2014).
For this reason, there is need to explore the philosophy that facilitate the staff to work in partnership at the St Andrew’s hospital. The philosophy is needed for several reasons but the ultimate goal is to providing quality care to the service users. The philosophy ensures that there is equity, quality and efficiency in the delivery of the healthcare and social care services. The philosophy is governed by ethics- a complex activity that is concerned with the moral obligations and dilemmas. Ethics in healthcare philosophy are governed by the ethical theories.
For example, the theory of deontology is concerned with the moral duty as well as the action rightness (Petch, Cook, and Miller 2013). Therefore, this theory suggests that a healthcare staff must always do what is morally right irrespective of the associated consequences. The other theory is the utilitarianism proposed by Jeremy Bentham, which is based on the principle of utility. Although these theories do not describe exactly on how a staff should behave, it gives the healthcare staff an understanding on how to motivate each other and pull ideas especially when confronted by ethical dilemmas and in accordance to ethical principles of autonomy, non-maleficence, justice and beneficence (Paterson, Nayda & Paterson 2012).
The working in partnership in health and social care at St Andrew’s hospital should be governed by the partnership philosophies such as respect, autonomy, and empowerment, power sharing, and making informed choices. The philosophy of empowerment involves sharing power with other partners who may not have the power. This philosophy is centered in healthcare service users and providers to enable them take greater charge of themselves.
It involves the process of recognizing, enhancing and empowering other people’s ability to meet their demands and to resolve their own issues with the available resources, making them feel in control of their lives. This enriching experience is associated with satisfaction and often leads to smooth partnership relationship (Robert& Cornwell 2011).
Certain populations in the society are said to be more vulnerable than others based on certain conditions or situations in life. The World Health Organization (WHO) defines high risk populations as individuals who cannot anticipate, resist, or cope and recover from the impacts of a disease or disaster. Elderly people, children, malnourished and immunocompromised individuals, and are all classified as high-risk population.
Some of the factors that have been attribute to expose people into vulnerability include poverty, poor housing, homelessness, ethnicity, race, genetic predisposition, as well as poor housing. Current economic indicators in the United States suggest that the most disadvantaged healthcare segments have been lagging behind despite overall increase in economic trends as well as that of racial, ethnic, and socioeconomic disparities.
For instance, the rates of infant mortality which have been falling for a number of years are now increasing among the African Americans; a trend that has been linked highly with poverty (Flynn et al., 2013). This has prompted the government to introduce some important health programs such as the Earned Income Tax Credit and the Social Security fund which have decreased poverty significantly induce major desirable health effects.
Nichols, O’Connor & Dunn, (2014) point out that DNP nurses play a crucial role of addressing and providing solutions in the healthcare field whose complexity keeps increasing. DNPs can impact a healthcare policy by solving disparities that surround the access to quality health care. Mostly, DNPs are the solution to a number of conflicting healthcare issues. One of the major roles that has been adopted by DNPs is identification of high-risk populations.
Predictive analysis has stood out as an important technique for effective identification. This method employs the use of historical and current data as well as modeling so as to predict future events. In predictive analytics, the decision-making process is data driven. Therefore, DNPs use available patient records to identify individuals that need assistance, such as high risk populations.
The African Americans are one of the high risk populations in America. This because of their high likelihood to develop hypertension. Researchers propose that these individuals could be carrying a gene that makes them salt sensitive hence increasing their risk to hypertension. Additionally, African Americans are affected significantly by obesity.
Studies by (Diaz et al., 2014) report that among non-Hispanic Blacks who are 20 years and above 77 percent of women and 63 percent of men are obese. This population also has a high prevalence of diabetes. It is important to note that diabetes and obesity are among the leading risk factors for hypertension and this could therefore be the reason behind the high incidence of hypertension among African Americans.
Evidence-based interventions
Several evidence-based interventions have been put forward to aid in the management of hypertension among the African Americans. One such intervention is the use of advance health care technologies. Technology advances have proven to be an integral part for the management of high-risk populations (James et al., 2014). For instance, technology will be used to support robust communication with high-risk individuals.
Text messaging, emails, social media, and video conferencing will be used by physicians to follow up on hypertensive patients so that they can understand their progress upon medical intervention. The technology will be used to enhance patient accessibility to healthcare. Additionally, health care providers can use remote monitoring or smart phones to optimize the healthcare strategies hence improving patient outcomes.
Another important intervention will be to education the African Americans about the etiology, causes, risk factors, and management of hypertension (Ogedegbe et al., 2014). There is need for patients to be enlightened about the importance of lifestyle changes. For instance, the African Americans will be encouraged to eat healthy foods such as the Dietary Approaches to Stop Hypertension (DASH) diet which stress that patients should take vegetables, fruits, fish, poultry as well as foods that are rich in potassium.
High levels of potassium aid in preventing and controlling high blood pressure. They should also regulate their intake of fats especially the trans-fat which has been proven to be responsible for arteriosclerosis that narrows blood vessels hence worsening hypertension.
Research has proven that one of the reasons behind the high prevalence of hypertension among black Americans is their increased sensitivity to salt (Diaz et al., 2017). Therefore, they should be educated about their need to reduce the intake of salt in their diet. A salt level of about 1500 mgs per day is recommended for a hypertensive patient who is about 50 years and above.
For other healthy individuals, advised not to increase their intake above 2000 mg as this could result in hypertension development. Obesity, smoking, and diabetes are other major risk factors that all African Americans will be taught about their management. They will be encouraged to present themselves to the healthcare centers for diabetes testing. Similarly, they will be encouraged to watch on their weight and desist from cigarette smoking as well as alcohol intake which can predispose them or increase the severity of hypertension.
The other strategy for managing and reducing hypertension will be by helping patients to design their hypertension treatment plan. Through this plan, patients will be instructed on how to check their blood pressure regularly, follow their treatment plans consistently, and consult their physicians regularly whenever need a clarification about their condition.
Outcome measurements
One of the measurements that will be used to evaluate the outcomes of the hypertension management is the recording of the mean systolic and diastolic pressure of the hypertensive patients who have been taught hypertension management interventions. The recording will be done over a period of one month and plotted on a graph where the shape of the graph will be used to determine whether the patient complied with what he/she learned.
The proportion of patients who will visit to the clinic after the education program will also be determine. A high turnout will be indicate that the patients understood that follow up care is an important pillar in the management of hypertension. Additionally, the physicians will use clinical records to determine how many more individuals have been diagnosed with hypertension since the implementation of the various evidence-based interventions. The number is expected to be lower compared to that of other years.
Epidemiological terminology in the description of interventions and outcomes
A systemic approach is required for effective management of hypertension. The approach entails identification of hypertensive patients, aggressive treatment of hypertension with antihypertensive drugs, proper patient education, and follow-up care. With this approach, modest reduction in the mortality and morbidity of cardiovascular agents will be realized.
However, it is important that note that all this strategies should be combined for clinically significant reductions in hypertension prevalence to be achieved. Supplemental interventions such as self-monitoring of hypertension and adoption of healthy behavior are other important indicators for use in assessing the effectiveness of the implemented strategies.
Lessons learned from developing this interventional program
This project has help me learn that communication is one of the most effective clinical intervention for use during management of a disease. Proper communication helps the public to understand the causes, risk factors, and their role in the prevention and management of a condition. Individuals who are well-informed know what they ought to do and therefore avoid visiting hospitals for treatment or hospitalization which is very expensive.
Secondly, I learned that healthcare providers should accord high-risk population optimum attention and conduct proper research in order to meet their desired goals. This is because interventions used in other parts of the world may not work when dealing with high risk populations hence the need of evidence-based programs. Through this intervention, I believe I can easily take care of an African American patient and also be at the front line in identifying other high risk-populations in the society and the clinical programs that can be used to ensure they live quality lives.
References
Diaz, K. M., Booth, J. N., Seals, S. R., Abdalla, M., Dubbert, P. M., Sims, M., … & Shimbo, D. (2017). Physical Activity and Incident Hypertension in African Americans. Hypertension, HYPERTENSIONAHA-116.
Flynn, S. J., Ameling, J. M., Hill-Briggs, F., Wolff, J. L., Bone, L. R., Levine, D. M., … & Ephraim, P. L. (2013). Facilitators and barriers to hypertension self-management in urban African Americans: perspectives of patients and family members. Patient Prefer Adherence.
James, P. A., Oparil, S., Carter, B. L., Cushman, W. C., Dennison-Himmelfarb, C., Handler, J., … & Smith, S. C. (2014). 2014 evidence-based guideline for the management of high blood pressure in adults: report from the panel members appointed to the Eighth Joint National Committee (JNC 8). Jama, 311(5), 507-520.
Nichols, C., O’Connor, N., & Dunn, D. (2014). Exploring early and future use of DNP prepared nurses within healthcare organizations. Journal of Nursing Administration, 44(2), 74-78.
Ogedegbe, G., Tobin, J. N., Fernandez, S., Cassells, A., Diaz-Gloster, M., Khalida, C., … & Schwartz, J. (2014). Counseling African Americans to Control Hypertension (CAATCH): cluster randomized clinical trial main effects. Circulation, CIRCULATIONAHA-113.
Want help to write your Essay or Assignments? Click here