Want help to write your Essay or Assignments? Click here
Breast Cancer Screening
Why is breast self-examination being replaced in the breast cancer screening guidelines by mammography and breast magnetic resonance imaging?
Breast cancer screening is normally done to facilitate early detection. This is important as it saves millions of lives in the world. According to guidelines by the American Cancer Society, breast screening should be done regularly. One of the most common and most easy methods is breast self-exam (BSE). This method has been advocated for in the recent past as it enables the women have sense of control over their breasts. Research highlights that over 70% of breast cancers incidences have been reported via BSE screening technique (Mahon, 2012).
However, there have been critiques on BSE screening method; especially due to increased incidences of benign biopsy. This is attributable to low specificity and sensitivity values. The excessive biopsies are associated with risk of cancer, emotional stress and disfiguring of the breast. The guidelines also tend to favour breast magnetic resonance imaging as well as mammography over breast self-exam method of breast screening. Magnetic resonance and mammography breast screening methods have high level of specify and sensitivity (Morrow, Waters, & Morris, 2011).
What are the risks associated with breast cancer screening? Do the risks outweigh the benefits? Why or why not?
Breast screening is important, especially for the woman in the case study as she is at high risk age. Breast screening involves process that aid in detecting breast cancer at early stage. Breast screening is done using many methods including mammogram, breast self-exam, and magnetic resonance imaging among others. Breast screening saves lives by ensuring that cancer is detected early, and appropriate interventions are made on a timely manner (Morrow, Waters, & Morris, 2011).
Want help to write your Essay or Assignments? Click here
However, there are risks involved in breast screening. To begin with, it is vital for a patient to understand that breast screenings does not prevent cancer. Some of the processes are uncomfortable and is associated with mild pain. Additionally, some processes involve use of X-rays- indicating that patients are exposed to radiation, which could lead to side effects.
However, the benefits outweigh the risks; therefore, every woman should be encouraged to undergo breast screening. There are many things that cause changes in the breast tissue. Although some of them could be harmless, it if important to get breasts checked as there is a small chance that the changes ignored are first indicator of cancer (Mahon, 2012).
References
Mahon, S. (2012). Screening for breast cancer: Evidence and recommendations. Clinical Journal of Oncology Nursing, 16 (6), 567-571. doi10.1188/12.CJON.567-571
Want help to write your Essay or Assignments? Click here
Migraine
Migraine occurs at all ages, but it is most common in the 3rd -5th decades of life. The prevalence rates are higher between 20-55 years, and peaks at age 40. Migraine is inherited. Most people suffering from migraines usually have family members that have them too. Research indicates that if one of parents suffers from migraines, there is a 50% chance that the child will suffer from migraines. If both patients suffer, the probability that the child will suffer from migraines increases to 75% (Bolay and Ertas, 2012).
The discussion explored the various types of headaches including rebound headaches and tension type of headache. The emerging theme from this discussion is the need to conduct complete history and physical assessments to rule out other causes of headaches. This includes the use of CT and EEG, their importance during diagnosis and monitoring disease progression.
However, these diagnostic tests should be conducted only if health assessments dictate so. It has been reported that headaches with aura increases a person’s risk factor for stroke. Therefore, it is important to assess patient risk to ischemic stroke, especially on women under hormonal replacement therapy and birth control tablets (Lampl et al., 2014).
Want help to write your Essay or Assignments? Click here
Most contributions on triggers have been mentioned. This includes fasting, stress, worry, menstrual periods, fatigue, head trauma, birth control pills, physical inactiveness, lack of sleep, hunger, and certain foods or drinks especially those that contain nitrites, tyramine, glutamate, and aspartate. Certain medications and chemicals substances have been found to trigger headaches, including estrogens, perfumes, nitroglycerin, hydralazine, and organic solvents with a strong (Rana et al., 2014).
The issue on treatment was also discussed. The main preventive strategies are lifestyle modification. NSAIDs such as ibuprofen, naproxen, and diclofenac are more effective as compared to aspirin or paracetamol. However, Triptans and Excedrin are more efficient for treating acute head attacks. Propranolol can also be prescribed if no contraindications are noted. Botox medications are effective for treating chronic migraines; usually used when all other treatment regimen is unsuccessful (Jackson, Kuriyama, & Hayashino, 2012).
Lampl, C., Jensen, R., Martelletti, P., & Mitsikostas, D. (2014). Refractory headache: One term does not cover all – A statement of the european headache federation. The Journal of Headache and Pain, 15(1), 1-2. doi:10.1186/1129-2377-15-50
Jackson, J. L., Kuriyama, A., & Hayashino, Y. (2012). Botulinum Toxin A for Prophylactic Treatment of Migraine and Tension Headaches in Adults. The Jouranl of American Medicine, 307(16), 1736-1745. doi:10.1001/jama.2012.505.
Rana, A. Q., Saeed, U., Khan, O. A., Qureshi, A. R. M., & Paul, D. (2014). Giant cell arteritis or tension-type headache?: A differential diagnostic dilemma. Journal of Neurosciences in Rural Practice, 5(4), 409-411. doi:10.4103/0976-3147.140005
Donnet, A., Daniel, C., Milandre, L., Berbis, J., & Auquier, P. (2012). Migraine with aura in patients over 50 years of age: The marseille’s registry. Journal of Neurology, 259(9), 1868-73. doi:http://dx.doi.org/10.1007/s00415-012-6423-8
Want help to write your Essay or Assignments? Click here
Want help to write your Essay or Assignments? Click here
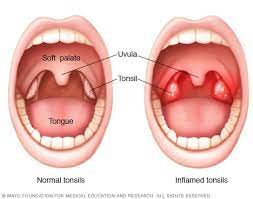
Tonsillopharyngitis Diagnosis
Patients presenting with sore throat and fever such as the one in question are primarily suspected for tonsillopharyngitis, whose primary cause is Group A Beta Hemolytic Streptococcus. Therefore, the diagnosis of acute tonsillopharyngitis relies on various tests such as white blood cell count (WBC), C-reactive protein (CRP), rapid antigen detecting test, and throat culture, a combination of which is called Center-Scoring or Clinical Scoring (Alper, 2013, p148).
This method can be well utilized in low income sections to prevent unnecessary use of antibiotics, which might lead to antibiotic resistance. Furthermore, Alper et al. (2013) give empirical data to support the reliability of this diagnosis procedure that is recommended in developed countries for being quick but efficient (p148).
Rapid antigen detection tests (RADT), as differential tests between viral and GAS tonsillopharyngitis, according to Toepfner et al. (2013) have gained a wide application in active diagnosis of group A streptococcal (GAS) tonsillopharyngitis. These include Rapid Agglutination Test or LAT and Lateral-Flow Immunoassay (p. 609). These tests have proved to be effective, this being the reason for the above state wide use in various countries, but they are sensitive and require prerequisite knowledge on how to conduct them accurately.
This is because according to a research done, comparing physicians and technicians, there is supported evidence that physicians may lack adequate technical knowhow when handling the tests. Often they might require an additional training before the results they deliver for the tests become reliable for any conclusions to be made in terms of whether Group A Beta Hemolytic Streptococcus tonsillopharyngitis infection is present or not. Technical errors, plus lack of experience and expertise have adverse consequences on accuracy of RADT (Toepfner, 2013, p609).
Want help to write your Essay or Assignments? Click here
An important aspect that comes out from the research done by Salatino et al. (2016) is that Rapid Streptococcus Test is the standard test, which is used by most physicians and Ear-Nose-Throat Specialists (p29). This method equivalently was found to allow for most diagnosis made per year, compared to other methods used for the same reasons. An important development is that there is common avoidance of antibiotic use in management of acute tonsillopharyngitis and other infections in the upper respiratory tract, due to the development of antibiotic resistance as earlier expounded on (Salatino, 2016, p29).
Alternatively, natural remedies which include homeopathy remedies are currently being used in complementary therapy. Tasar et al. (2015) note that an in depth examination of previously diagnosed cases of acute tonsillopharyngitis in children between the age of five to fifteen years, there is significant infections due to Group C and G streptococcus, though the most common presumption is that this infection is primarily caused by Group A streptococcus (p. 15). Therefore, it is always necessary to conduct differential diagnosis tests on throat cultures, when it comes to tonsillopharyngitis infections, in order to clearly put to record the type of streptococcus causing the infection.
Patient Care
Patient care for patients with acute tonsillopharyngitis encompasses to the various management approaches undertaken on both inpatients and outpatients. Al Alawi et al. (2015) state that, Outpatient parenteral antimicrobial therapy, or OPAT with ceftriaxone, is normally applied for treatment of acute tonsillopharyngitis (p279). This is applied on patients with infections that require medicines to be administered through the parenteral route and are adequately stable not to be admitted as inpatients (Al Alawi, 2015, p. 279).
This method according to this research is not only cost effective, but also saves bed spaces required for patient care and is found to reduce cases of acute tonsillopharyngitis infections by nearly half (Al Alawi, 2015, p279). Customer satisfaction is also recorded, with the administration of the drug being done at a minimum of three days in the clinic. This is an example of outpatient care and a reliable therapy that can be recommended for treatment of the acute condition in question, especially for if caused by streptococcal infections.
The OPAT treatment method began in USA around 1974 and has become a common mainstream practice (Al Alawi, 2015, p279). The treatment therapy is combined with the following aspects of patient care. Patients in the OPAT clinic are accorded close surveillance by officials who may be a family physician alongside a properly trained nurse (Al Alawi, 2015, p. 279).
Pharyngeal sterilization is also done using oral penicillin in the patient care before administration of IV ceftriaxone by the above named practitioners, who closely observe patient progress as the OPAT is undertaken. The patient is required before being put under the OPAT clinic care to be in safe social circumstances, such as have a telephone and means of transport in order to be able to rush quickly to the clinic in the event the illness becomes worse.
Want help to write your Essay or Assignments? Click here
Furthermore, patient safety is ensured in the care process by ensuring a close adherence to OPAT guidelines, as well as having a multidisciplinary team conducting the same which includes an infectious disease consultant, family physician, and a well-trained nurse (Al Alawi, 2015, p. 279). Proper interventions are initiated when any adverse effects or emanating complications are noted in the patients during their antibiotic intake.
Moreover, they are advised to report to the emergency and accident department at the clinic if any such effects are observed. During this period, fever recovery, sore throat period and number of returns to the clinic are assessed as the main markers of efficacy (Al Alawi, 2015, p. 279).
In patient care involves admission of patients who are dehydrated, have venous deficiencies or electrolyte imbalances. These are offered beds in the hospital, from where normal saline, dextrose, painkillers and antibiotics are administered intravenously. Oral penicillin is also given before ceftriaxone administration.
A similar assessment of efficacy is done in terms of dosage of drugs used versus fever recovery, sore throat relief period and time taken for the patient to gain stability. Once stable, the patients can be discharged with take home medicine to complete the relevant doses. This next step is normally follow up as discussed below.
Want help to write your Essay or Assignments? Click here
Follow Up
Vrca Botica et al. (2013) explain that there have been many reported cases of unnecessary prescriptions of antibiotics in diagnosis and treatment of acute tonsillopharyngitis (p440). In this regard, it is necessary to conduct follow up visits to ensure that there are no recurrent episodes of the infection, which might indicate improper prescription of the antibiotics maybe due to incorrect center scoring. Patient contacts should be kept in records of health in order to aid in communicating with the patient on the any follow up requirement by the physician.
Also, follow up notes should be taken and kept for future consultation plus decision making. These are important to elicit recurrence of the condition, which might dictate the type of prescription to be made in the future or even note some key details concerning the patient that were not covered during the earlier assessment. Significantly, follow up data collected can be used by a physician to assess the efficiency of a procedure applied in order to dictate using empirical evidence use or cessation such.
Another important element is the formulation of a follow up schedule for a patient post care assessment, which does not only keep the patient in the know about clinical follow up dates, but also enables a physician to arrange his or her schedule in a manner as to meet all follow up requirements. Gupta et al. (2015) report of a monthly follow up on a patient who had tonsillopharyngitis caused by EBV. Therefore, it is important for the physician involved to decide wisely on the time period that he or she will conduct the follow up, more conveniently with specific objectives in mind though flexibility will be best if embraced.
Sometimes it might require follow up in terms of throat culture RADT to ensure no recurrence of GAS related tonsillopharyngitis infection is recorded. Progress during the follow up in terms of the rapid test results can be tabulated, graphically analyzed and interpreted to give the management therapy a deeper insight into effectiveness of methodologies applied.
A secondary center scoring can also be done and the results manipulated in a similar fashion to obtain specific desired outcomes. This implies that follow up is outcome based, should be planned for appropriately with holistic patient involvement, and records on the same should be well documented or kept together with other health records for future consultations.
Patient Education
Tonsillopharyngitis is a condition that can be managed easily. Patients should be sensitized on the primary symptoms of tonsillopharyngitis so that they can seek medical attention at the right time before the condition progresses and becomes difficult to manage. Some of these symptoms include runny nose, fever, cough, and watery eyes.
Moreover, patients should be educated on how the condition is acquired so that they can refrain from exposing themselves in environments that put them at risk of acquiring tonsillopharyngitis infection as well as how they can stop the spread of this condition to their family members and friends. By so doing, the prevalence of tonsillopharyngitis will decrease considerably.
Alper, Z., Uncu, Y., Akalin, H., Ercan, I., Sinirtas, M., & Bilgel, N. G. (2013). Diagnosis of acute tonsillopharyngitis in primary care: a new approach for low-resource settings. Journal of Chemotherapy, 25(3), 148-155.
Bélard, S., Toepfner, N., Arnold, B., Alabi, A. S., & Berner, R. (2015). β-hemolytic streptococcal throat carriage and tonsillopharyngitis: a cross-sectional prevalence study in Gabon, Central Africa. Infection, 43(2), 177-183.
Salatino, S., & Gray, A. (2016). Integrative management of pediatric tonsillopharyngitis: An international survey. Complementary Therapies in Clinical Practice, 22, 29-32.
Tasar, M. A., Bostanci, I., Karakoc, A. E., Selver, B., Demirbilek, M., & Dallar, Y. (2015). Prevalence of group C and G streptococcus in pediatric acute tonsilopharyngitis in Turkey. Group, 14, 15.
Toepfner, N., Henneke, P., Berner, R., & Hufnagel, M. (2013). Impact of technical training on rapid antigen detection tests (RADT) in group A streptococcal tonsillopharyngitis. European journal of clinical microbiology & infectious diseases, 32(5), 609-611.
Vrca Botica, M., Botica, I., Stamenić, V., Tambić Andrašević, A., Kern, J., & Stojanović Špehar, S. (2013). Antibiotic prescription rate for upper respiratory tract infections and risks for unnecessary prescription in Croatia. Collegium antropologicum, 37(2), 449-454.
Want help to write your Essay or Assignments? Click here