Want help to write your Essay or Assignments? Click here
SOAP Note for a Patient with; Ectopic Pregnancy
Subjective
A 30-year-old female, gravid 1, para1+0.The patient complained of abdominal pain in the right adnexal area which was generalized. She complained of dizziness, light headedness, and syncope. She experienced abnormal uterine bleeding for three days. She had not undergone and gynecological operation and had been on folic and iron supplements. Her menarche was at the age of 14years. Her menses were regular and used to last for 5days and occurred every 28days.The patient had used hormonal implant for three years and had been removed three months ago. She had not received her menses for two months. She was sexually active and had post-coital bleeding. She used to take alcohol on a regular basis.
Objective
The patient was sick looking and was groaning in pain.On palpation, there was generalised abdominal tenderness, and unilateral adnexal mass was present on the right hypochondria. Her vital signs were; Temperature -36.7degrees Celsius, blood pressure-98/56 mm/Hg, pulse-50beats/min. On bimanual examination, there was cervical motion tenderness. Her Serum HCG levels were 4500 IU/l; a trans-vaginal Ultrasound revealed a tubal mass in absence of intrauterine gestational sac.
Assessment
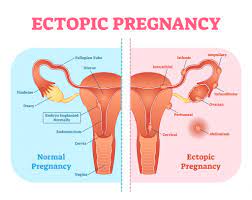
- Ectopic pregnancy which leads to acute abdominal pain and bleeding (Marion & Meeks, 2012).
- Ovarian torsion resulting in localized lower abdominal pain radiating to the back or thigh and nausea and vomiting
A Urinary tract infection leading to lower abdominal pain and dysuria and increased micturition
- Appendicitis presenting with guarding abdominal pain and nausea and vomiting. Diagnosis of ectopic pregnancy was made due to the acute abdominal pain, associated bleeding, and increased βhCG levels
Plan
The overall goal of management was to preserve the life of the mother, and this was managed through termination of pregnancy and reconstruction of the implantation site. The patient was given a bed rest ensure that she had reduced activity (Marion & Meeks, 2012). The patient was cannulated and started on intravenous fluids to restore the fluid volume deficit. Blood samples for the laboratory were obtained. Relaxation techniques were used to relieve pain.
Want help to write your Essay or Assignments? Click here
Medical management
The patient was put on intramuscular methotrexate. Methotrexate is a folic acid antagonist which deters cell division. The products of conception degenerates and detaches from the uterus leading to death (Epee-Bekima & Overton, 2013). Viability of the cytotrobhoblast is prevented together with β-hCG secretion (Wright, Busbridge & Gard, 2013).
Surgical management
Laparoscopic salpingectomy was considered to be the primary treatment of the ectopic pregnancy. Salpingectomy was conducted so as to repair the ruptured fallopian tube (Marion & Meeks, 2012).
Alternative management
Expectant management, the ectopic pregnancy could be waited to resolve on its own. However, this would be followed by β-hCG measurement and trans-vaginal ultrasound to confirm whether the disorder has resolved (Epee-Bekima & Overton, 2013).
Follow-up
The patient was advised to visit the clinic after 3-4 weeks for b-hCG measurement and ultrasonography. The patient was also advised on early pregnancy clinic visits.
Reflection notes
Patient involvement: I would carefully advise my patient of the advantage associated with any of the treatment approaches and ensure she fully participates in the selection of the mode of therapy. The use of laparoscopy could be used so as to come up with the diagnosis so as to minimize use of Surgery is the primary form of treatment. In addition to that, a less surgical procedure such as laparoscopic approach would have been used since it is associated with minimal intra-operative blood loss and hospital stay.
References
Epee-Bekima, M., & Overton, C. (2013). Diagnosis and treatment of ectopic pregnancy. The Practitioner, 257(1759), 15-18.
Marion, L. L., & Meeks, G. R. (2012). Ectopic pregnancy: history, incidence, epidemiology, and risk factors. Clinical obstetrics and gynecology, 55(2), 376-386.
Mergenthal, M. C., Senapati, S., Zee, J., Allen-Taylor, L., Whittaker, P. G., Takacs, P., … & Barnhart, K. T. (2016). Medical management of ectopic pregnancy with single-dose and 2-dose methotrexate protocols human chorionic gonadotropin trends and patient outcomes. American Journal of Obstetrics and Gynecology.
Practice Committee of the American Society for Reproductive Medicine. (2013). Medical treatment of ectopic pregnancy: a committee opinion. Fertility and Sterility, 100(3), 638-644.
Wright, S. D., Busbridge, R. C., & Gard, G. B. (2013). A conservative and fertility-preserving treatment for interstitial ectopic pregnancy. Australian and New Zealand Journal of Obstetrics and Gynaecology, 53(2), 211-213.
Want help to write your Essay or Assignments? Click here
